Diseases Of The Joint And Bursae
Description
This section is from the book "Applied Anatomy: The Construction Of The Human Body", by Gwilym G. Davis. Also available from Amazon: Applied anatomy: The construction of the human body.
Diseases Of The Joint And Bursae
The shoulder-joint, like other joints, is subject to inflammatory and other diseases. These may be (1) traumatic and later septic; (2) rheumatic or gouty; (3) tuberculous, with suppuration.
These affections result in an effusion within the joint-cavity which distends the capsule and finally tends to escape at the weakest points. The joint is not a complicated one, like the knee, and its synovial membrane is neither so extensive nor so elaborate.
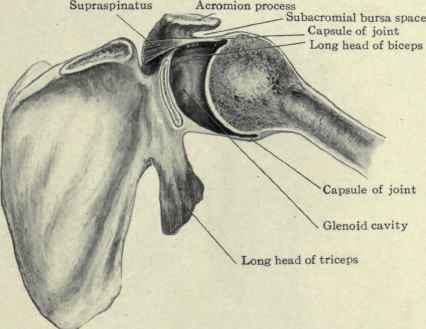
Fig. 266. - Transverse section of shoulder-joint, illustrating the laxity of the capsule of the joint.
Traumatism may give rise to a synovitis, an inflammation of the synovial membrane, or an arthritis involving the entire joint structures. Sprains and other injuries are not uncommon. A sprain will be caused by a force which acts to a greater extent than the normal movements of the joint will allow.
Movements Of The Joint
In abduction the capsule becomes tense at its lower portion when the arm is at 90 degrees to the trunk, greater abduction is resisted by the greater tuberosity impinging on the acromion process and the scapula begins to revolve.
Adduction is resisted both by the muscles and by the ligaments. When the ligaments only remain, the head can be separated for 2 cm. or more from the glenoid cavity (see Fig. 266). Marked adduction is usually limited by the arm coming in contact with the side of the body.
If the humerus is brought diagonally across the chest the scapula begins to move and its posterior edge and lower angle turn forward. As the humerus is adducted the deltoid and supraspinatus are made tense and the head is drawn up in its socket. When the muscles are paralyzed the weight of the upper extremity allows the head to fall and a distinct depression can be seen beneath the acromion process. In paralysis of the deltoid this is particularly noticeable.
If traction is made on the arm, the muscles are the resisting agents. If the arm is in a position of adduction, those going from the humerus to the scapula, as the deltoid, supraspinatus, biceps, and triceps, act. If in abduction, then also those from the humerus to the trunk, like the pectoralis major and latissimus dorsi, are brought into play. The part played by the deltoid and trapezius should be noted. If the arm is down by the side and traction is made on it, the force is transmitted from the humerus in a direct line through the deltoid and the upper fibres of the trapezius to their attachment to the spine and superior curved line of the occiput. If, on the contrary, the traction is made while the arm is raised above the level of the shoulder, the force is transmitted through the axillary fold muscles as well as by the deltoid and continued through the lower fibres of the trapezius. In either case the muscles are the resisting agents and not the ligaments. Abduction to more than a right angle is resisted by the contact of the greater tuberosity with the under surface of the acromion process and coraco-acromial ligament and the under side of the capsular ligament is made tense. The raising of the arm to 90 degrees is performed by the supraspinatus and deltoid muscles of the scapula and beyond this by the serratus anterior and other muscles.
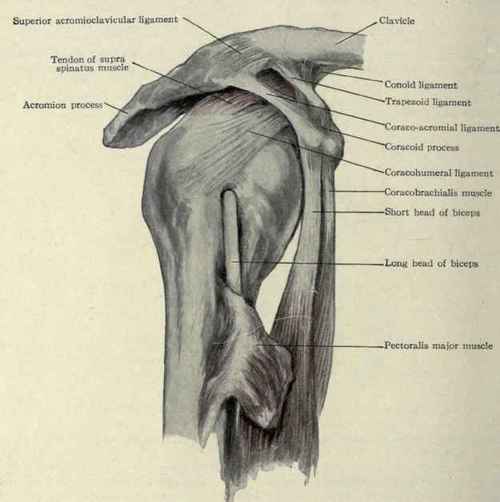
Fig. 267. - Acromioclavicular and shoulder joints.
Inward rotation is limited by the infraspinatus and teres minor muscles and by tension of the upper portion of the capsule. Outward rotation is limited by the sub-scapularis and upper portion of the capsule. The humerus rotates on its long axis 97o (Macalister).
Continue to:
My Books

