The Pericardium. Continued
Description
This section is from the book "Applied Anatomy: The Construction Of The Human Body", by Gwilym G. Davis. Also available from Amazon: Applied anatomy: The construction of the human body.
The Pericardium. Continued
Paracentesis Of The Pericardium
Tapping the pericardium by means of a trocar or aspirating needle must be carefully done, or the pleura may be punctured.
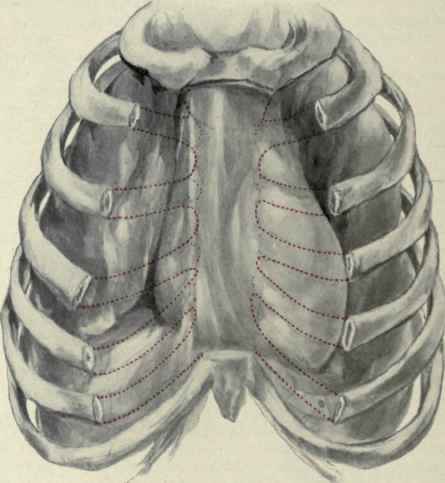
Fig. 218. - View of the pericardium, slightly distended, and its relations to the bony thorax.
The part of the pericardium in contact with the chest-wall which is never covered by pleura is small. It embraces the space between the two pleurae from the fourth to the seventh ribs. This may be defined by three lines, one in the midline, another from the middle of the sternum opposite the fourth rib to the costosternal junction of the seventh rib, and a third joining these two passing through the articulation of the xiphoid cartilage (Fig.219).
The left pleural sac may be 1 cm. distant from the left edge of the sternum. Thus it is seen that there is hardly a point where a needle can be introduced with the certainty of avoiding the pleura. The safest point is probably close to the left edge of the sternum in the sixth interspace. This interspace may not extend to the sternum, but even if the cartilages are in contact a needle could probably be introduced at this point. As the pericardium is distended it carries the lungs and to a less extent the pleura outwards and increases the area available for puncture both upward and downward as well as to the sides. When greatly distended the pericardium may reach to the first interspace above, 2.5 cm. (1 in.) to the right of the sternum, to the seventh cartilage below, and to the left nipple line or even beyond. The arching of the diaphragm causes a sternophrenic sinus behind the sternum analogous to the costophrenic sinus at the lower edge of the chest. This becomes distended by pericardial effusions in the same manner as does the costophrenic sinus in pleural effusions. A puncture in the sixth space close to the left edge of the sternum enters this sinus. The increased area in cases of distention from pericardial effusions has led Osier to advise tapping in the fourth interspace, either at the left sternal margin or 2.5 cm. from it, or at the fifth interspace 4 cm. (1 1/2 in.) from the sternal margin; or by thrusting the needle upward and backward close to the costal margin in the left costoxiphoid angle.
It is important to avoid wounding the internal mammary artery, which is usually nearer to the sternum above (0.5 to 1 cm. to its outer side) and farther from it (2 to 3 cm.) below.
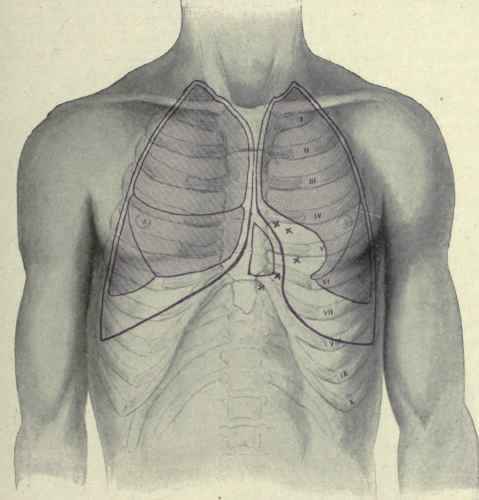
Fig. 219. - Paracentesis of the pericardium.
The danger of wounding the pleura in aspirating with a needle has probably been overestimated, but when drainage is to be employed the danger is certain.
Drainage Of The Pericardium
To drain the pericardium requires the removal usually of at least one of the costal cartilages. A drainage-tube can sometimes be introduced by first making a short incision in the fifth or sixth interspace close to the left edge of the sternum, then puncturing the pericardium, dilating the puncture with forceps, and introducing the tube. The costal cartilages usually lie so close together as to interfere with the proper introduction of a tube, hence the necessity of resection. A flap may be made or a straight incision. The latter is sometimes made over the fifth costal cartilage, which is then resected. If desired the sixth and seventh cartilages are also removed and even a piece of the left edge of the sternum. The intercostal muscles having been raised, the cartilages are removed.
When the internal mammary artery is seen lying beneath, it is to be either ligated or drawn to one side. The triangularis sterni muscle is either incised or drawn to the outer side along with the edge of the left pleura. The pericardium can then be lifted with forceps and incised and the drainage-tube introduced.
Continue to:
My Books

