8. Home Nursing. 2. Nursing Accident Cases
Description
This section is from "Every Woman's Encyclopaedia". Also available from Amazon: Every Woman's Encyclopaedia.
8. Home Nursing. 2. Nursing Accident Cases
Continued front page 2659, Part 22
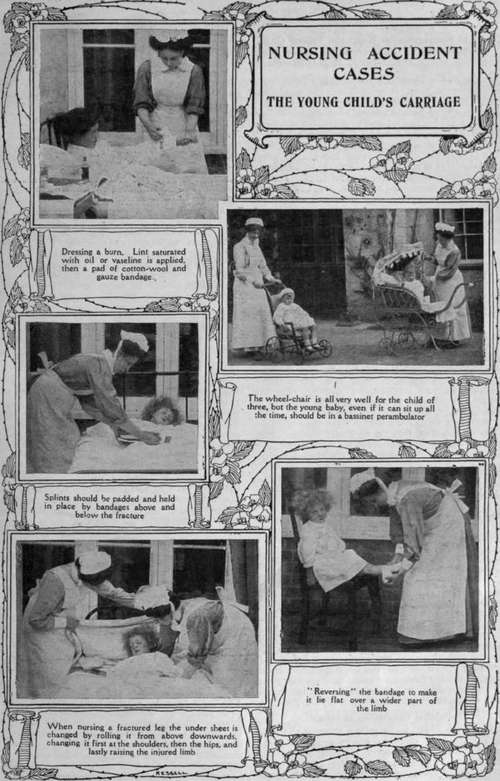
The Treatment of Burns - Three Classes of Burns - How to Prevent Contraction During Healing - Nursing of Fractures - Adjustment of Splints - Undressing the Patient - "Reversing" a Spiral Bandage
The amateur nurse will very probably be called upon to take charge of many ordinary cases of burns in the home. Wherever there are children, burning accidents are liable to occur, whilst the cook who does not occasionally sustain a burn in the process of her work is exceptional.
Whenever a severe burning accident occurs a doctor should be summoned at once. A burn over a large area, even if it is not very deep in extent, is always accompanied by shock, and children and old people are especially liable to collapse from this cause.
Burns, And Their Treatment
The first-aid treatment of burns has been considered (page 743, Vol. 1). It simply remains to emphasise the fact that the more quickly the air is excluded from a burn, and it is dressed with some oil or greasy substance, the better. Even more important it is to counteract shock by keeping the patient warm, and giving hot drinks, and even stimulants, if he is conscious. The amateur nurse must realise the gravity of burns, and remember that although the patient does not complain of much pain, after-collapse may happen at any moment from failure of the heart. The subject will be more readily understood if we divide burns into three classes.
1. In burns of the first degree the skin is simply reddened and congested because the burn. is superficial. There is a good deal of pain with these slighter burns because the uppermost layer of the skin is destroyed, and the nerve endings in the true skin underneath are exposed to the air.
2. Burns of the second degree show the skin raised into blisters, and in the case of such a burn much damage is apt to be done by carelessness in removing the clothing.
3. Burns of the third degree show destruction of the skin in the tissues underneath to a varying depth.
Treatment rather depends upon the type of burn, and the amateur nurse has considerable choice with regard to the materials she uses. Anyone who is following these articles in the right spirit has in her first-aid cupboard all the necessary materials for treating burns in emergency. For first-aid purposes it will be necessary to cover the burns with ointment, vaseline, or oil, as quickly as possible until the doctor arrives. The nurse, however, who has charge of the burning case, has every day to give her attention to the dressing of the burn, as well as to the general condition of the patient. It is not necessary, as a rule, that anyone who has sustained a burn of the first degree, unless it is over a very large extent of surface, should be put to bed. The part is simply dusted with boracic powder or even flour, and covered with lint and a bandage. When there is a good deal of pain, however, and a considerable area of skin is affected, it would be much better to dress this burn with carbolic oil applied on lint.
In the more severe burns, where the skin is raised into blisters, the best treatment is boracic ointment with a thick covering of lint covered with a pad of wool and a bandage. The vesicles may require to be opened with a needle, which has been boiled to sterilise it or make it perfectly "clean." The important thing for the nurse to attend to in dressing these burns is to prevent the entrance of microbes. The vitality of the tissues is so much depressed after burning that suppuration is very apt to occur unless the part is kept absolutely clean.
A doctor will be in charge of burns of the third degree, so that it will be sufficient if the nurse carefully follows his instructions with regard to dressing them. Iodoform will probably be used as an ointment, with vaseline, and the wound will be covered with antiseptic wool and a bandage.
As a rule, burns are dressed as seldom as possible, because unnecessary exposure of the burnt part to the air causes considerable shock to the patient; and the nurse - has a very responsible duty in nursing burns to prevent contraction or after-deformities. A badly-dressed burn of the hand, for instance, may be followed by a deformity in which the fingers are drawn down towards the palm, or burning of the neck may be complicated with the head attracted to one side. These deformities can all be avoided if the nurse is careful in dressing the case during healing, and if the doctor is called in at once should anything go wrong.
Some General Hints
In nursing any case of burns the nurse has to be especially careful that the patient takes food and stimulants regularly. After the first shock of collapse has been overcome, the patient's spirit must be kept up by giving plenty of nourishment, with whatever stimulants the doctor orders at definite hours. At the beginning of the illness the patient will probably be given milk, broth, and beef tea, which is an excellent stimulant, although it does not contain a great deal of nourishment. Whenever he is able to take more solid food, eggs, milk, and cream foods should be administered, and the patient encouraged to take as much nourishment as possible.
One of the best medicines in the treatment of burns is sleep. The shock to the nervous system is very great, and only by regular, quiet sleep can the patient's nerves recover tone and vitality. An afternoon sleep should be insisted upon, and the patient made ready for the night by nine o'clock. Nourishment may be required during the night, and in such cases one of the patent heaters for keeping liquid food warm should be used. This is usually supplied by a Pyramid night light, which will last for eight hours, and keep the food hot and ready for use.
The patient will probably suffer from thirst, and cold water should be given in small quantities at a time, or teaspoonfuls of cold coffee. A little lemon-juice is an excellent thing for counteracting thirst, and the nurse should be careful to keep the mouth quite clean by using such a mouth-wash as a few drops of tincture of myrrh, and half a teaspoonful of borax in a teacupful of tepid water.
The Nursing Of Fractures
After the doctor has "set" a fracture the nurse in charge has to attend to special points. She must note accurately the position in which the splint is applied, in order that she may be able to notice any shifting of the splints. When a doctor sets a fracture he simply puts the limb into the natural position, and keeps the bones in this position until the two ends of fractured bone are joined together again. This he achieves by splints, pieces of wood of special size and length which are long enough to fix the joints above and below the seat of fracture, in order to prevent any movement.
The nurse must know how to pad these splints properly so that there is no pressure of the hard wood upon any part of the limb. Splints should always be padded evenly with tow, cotton-wool, old soft linen, or lint. The nurse has to see that the splint is quite flat when padded, and that it is a little wider than the limb.
All creases and folds must be avoided, as they are uncomfortable to the patient and may produce sores on the skin. Supposing a fractured leg has been put up in splints, the nurse must watch if the heel is exposed, and that a bed-sore does not form on it from pressure. A small pad of cotton-wool or tow should be placed between the heel and any splint. The nurse should also keep a sharp look-out upon the fingers or toes for any blueness, coldness, or swelling, which are signs that the circulation is being obstructed somewhere. In such a case the splints will have to come off and be reapplied.
When undressing an accident case the first principle is that the clothes should be taken "away from the patient, not the patient away from the clothes."for example, if an arm is injured the sleeve of the sound arm should be taken off first and then the injured arm dealt with. If the leg is injured the trousers will have to be slit up the outer side. The boot will have to be cut away down the back seam and through the laces, and the sock cut off in the same way.
The great aim should be to keep the patient as still as possible. In hospital, sand-bags would be used to put on either side of the injured limb to keep it steady, but the amateur nurse will probably have to use pillows and bolsters on either side to keep the injured part at rest whilst she is removing clothing from the patient. After a fracture is set, and the patient made comfortable, a "cradle" must be placed over the injured limb to keep the blankets oft the part. Two halves of a hoop will answer the purpose. A three-legged stool or a hatbox will make an excellent temporary cradle for keeping the bedclothes away from the limb. A bandage should never be applied over the site of a fracture or between the splints and the limb, or gangrene may follow.
A Few Rules for Nursing Fractures
1. Always work at the same side of the bed as the injured limb.
2. Take hold of the limb by sliding the fingers below until it rests upon the hand.
3. Have everything ready for the doctor in the way of fresh padding, bandages, etc., if he intends to look at the fracture.
4. If the doctor wishes the fracture to be massaged after the first few days, ask for definite directions as to how this is done. A subsequent article will deal with the subject of massage.
5. Impress upon the patient the need of absolute rest if the fracture is to heal quickly.
6. In changing sheets the under sheet must be rolled from above downwards, changing the sheet first at the shoulders, then at the hips, and lastly raising the injured leg. The new sheet is rolled into place as the old one is rolled off.
Bandaging Lesson
By now the amateur nurse has practised applying the bandage circularly round the limb. This is called the "spiral bandage," and now we must consider how to put on a bandage carefully over the limb when it begins to increase in thickness. If the spiral is simply worked up in this way the bandage would not lie flat, but it would be all uneven and loose. So that when you come to a thicker part of the limb the bandage must be reversed. When standing in front of the patient, with a roller bandage in the right hand, the thumb of the nurse's left is pressed upon the lower border of the bandage, which is twisted downwards so that it is reversed and is then passed round the limb once more. These reverses are made right up the limb, to the elbow or knee, as the case may be. The next lesson in bandaging will describe how to bandage joints by means of the " figure of eight."
Continue to:
My Books

