Diseases Of The Liver
Description
This section is from the book "A Manual Of Pathology", by Guthrie McConnell. Also available from Amazon: A Manual Of Pathology.
Diseases Of The Liver
Malformations are not common and seldom of importance. Complete absence is seen in acardiac monsters. Variations in the number of lobes and in the fissures may occur. Portions of hepatic tissue may be separated from the main mass, but are usually connected by a pedicle of connective tissue. Malformations may be acquired particularly as a result of tight lacing, which causes a deep transverse notch upon the anterior surface which may almost divide the organ, the hepatic tissue along the line of pressure undergoing atrophy.
The position of the liver may be changed by relaxation of its ligaments or by pressure from tumors within the abdomen.
The ribs posteriorly and the right crus of the diaphragm may by pressure form long furrows.
Disturbances Of Circulation
The liver is peculiar in its blood-supply in that it contains two systems. One of these, the lesser, supplies nutrition to the stroma; the other, which is of much greater importance, supplies the blood necessary for the carrying on of the hepatic functions. This latter, the portal system, divides into many branches that ramify throughout the acini and empty into the central veins of the lobules, branches of the hepatic. The blood flows very slowly through the organ and is under very little pressure, consequently is readily interfered with by slight obstruction.
Anemia may be part of a general anemia or may be due to pressure upon the blood-vessels. The organ is pale, but may vary in color according to the amount of bile or of fatty degeneration present.
Active Hyperemia
Active Hyperemia occurs normally during digestion, and is also present as an accompaniment of inflammation, in which case the areas are circumscribed. May be general as a part of an infectious process. The organ is slightly enlarged, softer, dark red in color, and on section blood readily escapes.
Passive Hyperemia
Passive Hyperemia is of greater pathologic importance than the active. It is caused by interference with the escape of the blood into the vena cava. Is found in valvular diseases of the heart, in those conditions interfering with the pulmonary circulation, as emphysema, chronic fibroid phthisis, etc., and may be due to pressure upon the vena cava by tumors. Pleural effusions with adhesions may cause it.
As a result of the obstruction to the circulation the central vein of the lobule first becomes dilated, and subsequently the capillaries in communication. Following this continued pressure there is atrophy of the cells in the central zone and at times even of those as far out as the periphery of the lobule.
The organ is at first enlarged, the anterior edge rounded, and may be darker in color. On section is seen the characteristic reddish-brown and yellow mottling known as the "nutmeg liver." The congestion of the central vein and its adjacent capillaries produces a reddish-brown central zone in the lobule. Next comes a zone in which atrophic pigmented liver-cells remaining between the dilated capillaries cause a brownish color. Still further toward the periphery of the lobules is a pale yellow zone of liver-cells that have undergone fatty degeneration. This area will frequently show some bile stasis.
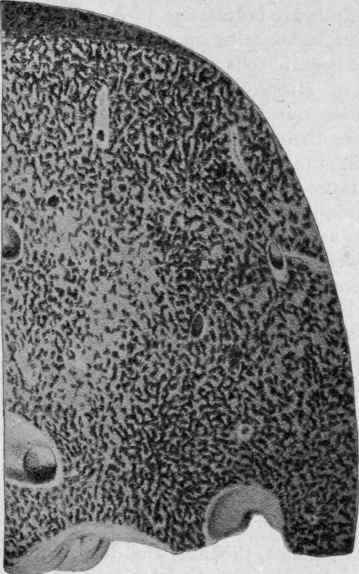
Fig. 156. - Nutmeg Liver: Chronic Congestion due to Cardiac Disease (Bollinger).
"The microscopic examination shows that in the early stages the intralobular venules and capillaries are dilated and overfilled with blood, the dilatation extending a variable distance toward the periphery of the lobules, depending upon the degree and duration of the process. The blood content of the capillaries consists not infrequently of a disproportionate number of leukocytes, which may be interpreted as evidence of stasis. More or less extensive hemorrhage into the centers of the lobules and consequent destruction of the hepatic parenchyma is not uncommon. It is found especially in cases of acute heart failure and in cases of chronic failure of compensation terminating in a sudden and complete breakdown. The hepatic cells about the central vein show a varying degree of atrophy - partially a pressure atrophy, and partly doubtless nutritional, the result of insufficient oxidation. In most cases there is a considerable accumulation of fat in the liver cells; in some cases this is excessive and accounts for the term "fatty nutmeg" liver. Usually the cells about the central venules contain more or less pigment derived from hemoglobin, usually in the form of hematoidin, but hemosiderin, as well, may be present".
If the congestion has been present for a long time the organ may become smaller, on account of atrophy of the hepatic cells, and firmer. The surface of the liver becomes uneven, due to hyperplasia of connective tissue, and is darkly pigmented, a condition known as cyanotic induration.
In some cases there is a deposit of hematogenous pigment throughout the organ, causing it to be dark red. Such a change is spoken of as red atrophy, as the liver is smaller than normal.
As a result of chronic congestion the action of the liver may be much interfered with, one of the most common symptoms being slight jaundice, probably due to the obstruction of the bile-ducts and capillaries by the swollen endothelial cells. The bile is also generally more viscid than normal.
Continue to:
My Books

