Leprosy
Description
This section is from the book "A Manual Of Pathology", by Guthrie McConnell. Also available from Amazon: A Manual Of Pathology.
Leprosy
Leprosy is a chronic, specific, infectious, inflammatory disease caused by the Bacillus leprae, which is a non-motile, non-sporogenous, acid-resisting, purely parasitic organism. It is pathogenic for man, but some of the lower animals appear to be somewhat susceptible. Is very slightly contagious. Is stained with some difficulty. Stains by Gram's. An acidfast organism supposed to be the B. leprae has been grown on artificial culture-media containing split-up nucleoproteins.
It occurs most commonly in warm climates and in people of almost any age. Is most common in males of from twenty to thirty years. It is probably not hereditary, but children under three years have been affected. Infection may be transmitted by: (I) direct inoculation; (2) kissing and sexual intercourse; (3) clothing; (4) bites of insects.
The bacilli are distributed to an extraordinary extent in the body of the leper, and in many cases there will be no inflammatory reaction in their neighborhood. They may be either extracellular or intracellular, and in the latter case may be found in giant cells or lepra cells. These may contain numerous nuclei and numbers of vacuoles as well as bacteria. The secretions of the numerous membranes of the nose usually contain great numbers of the bacilli.

Fig. 30. - Giant Cell from a Leprous Ulcer of the Epiglottis, Showing the Lepra Bacilli Scattered Through the Tissue and Enclosed in a Large "Lepra Cell" (Lehmann and Neumann).
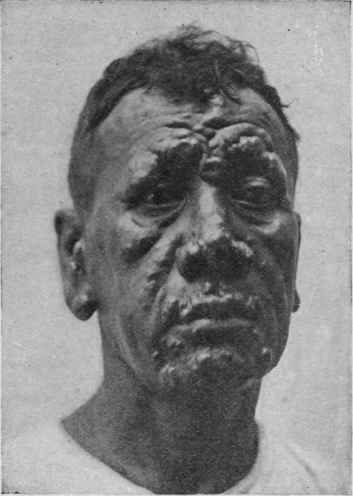
Fig. 31. - Nodular Leprosy.
Varieties
Two forms are commonly met with, the nodular and the anesthetic or nerve leprosy. It is seldom, however, that a quite pure case of either is found; the majority belong to the mixed form. In the nodular variety the node may be preceded by a hyperemic patch which leaves behind it a pigmented area. The nodules appear first in the skin and subcutaneous tissue of the face, and may remain single or become confluent.
Macroscopically the nodes are rather grayish or yellowish.
Microscopically each node is made up of granulomatous tissue composed of lymphoid and epithelioid cells retained in a loose connective-tissue network; in these masses the bacilli occur in great number between and in the cells. These lesions are more vascular than those of tuberculosis, and consequently do not tend to undergo coagulation necrosis. Caseation does not take place and the ulceration that is so common depends largely upon injuries and secondary infections.
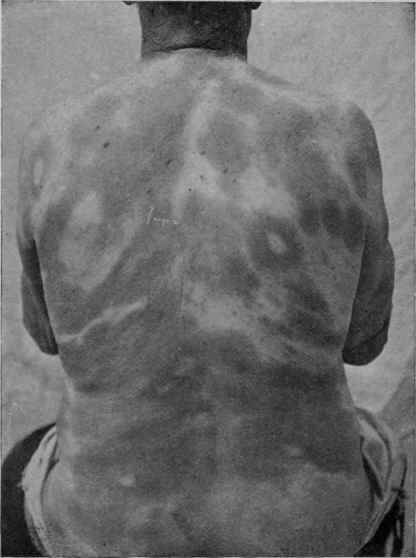
Fig. 32. - Macular Lesions in Anesthetic Leprosy.
The nodules are found in other parts of the body, as on the back of the hand, - palm is not usually involved, - in the mucous membrane of the eye, nose, mouth, larynx, and intestines.
The lymph-glands in both varieties are swollen, hard from connective-tissue formation, and yellowish on account of fatty degeneration.
Anesthetic leprosy is characterized by the growth of the bacilli in the sheath of the nerves and an increase in the connective tissue along their course. Is most common on the ulnar and popliteal nerves, which at first may be painful. There then appears neuritis with localized hyperemic spots, the nerve affected being red and swollen; later it becomes harder, pale, and gray, with nodular or fusiform enlargements. The neurilemma usually becomes thickened, fibrous, and infiltrated by cells and bacilli. These become anesthetic, and in some cases become the seat of a blister. Finally, ulceration may develop with the subsequent loss of the fingers or toes.
Many of the enlarged nodes may be the result of a secondary-tuberculosis occurring late in the course of the disease. There is frequently fever and also nephritis. Amyloid degeneration is not uncommon in the ulcerative forms.
The majority of the cases last from five to twenty years, usually dying of tuberculosis.
Continue to:
My Books

