X-Ray Studies of Of The Colon And/Or Rectum Cancer. Continued
Description
This section is from the book "Early Detection And Diagnosis Of Cancer", by Walter E. O'Donnell. Also available from Amazon: Early Detection And Diagnosis Of Cancer.
X-Ray Studies of Of The Colon And/Or Rectum Cancer. Continued
(c) The summit of the lesion is the portion most likely to prove suitable for partial biopsy. The pedicle should be avoided in a partial biopsy because of the likelihood of bleeding.
(d) A small-mouthed biopsy forceps of the type shown in Fig. 73 is recommended.
(e) Local pressure and Celfoam usually suffices to stop bleeding.
5. Examine all tissue removed pathologically. A "benign-appearing" lesion may contain microscopic carcinoma. Proper treatment is dependent on exact knowledge of the lesion's potential.
6. Remove all polyps in their entirety.
(a) In the case of small lesions, total excision with the biopsy forceps may prove adequate provided the pathology report is benign.
(b) For larger lesions, wherein the biopsy is benign or shows atypical epithelium, cautery snare removal with fulguration of the base may be adequate therapy. This may hold true also for carcinoma confined to the summit without histologic evidence of invasion of the stalk.
(c) When pathologic examination suggests invasion of the stalk, base, or beyond the base, bowel resection is usually required.

Fig. 73. Universal biopsy forceps for the biopsy of rectal lesions.
(d) Small areas of hyperplasia may be excised or kept under periodic observation.
7. Re-examine the patient with the sigmoidoscope at six-month intervals for one to two years and then annually.
8. Repeat the barium enema with air contrast study after one year and, if negative, every two years thereafter.
If a high-lying polyp is found in the colon above the reach of the sigmoidoscope:
Such a lesion is usually seen on x-ray examination prompted by (1) the finding of a low-lying polyp in an asymptomatic individual, (2) blood or mucus coming from above noted on sigmoidoscopy, (3) unexplained lower bowel symptoms.
1. Repeat the barium enema with air contrast study.
(a) Since a recommendation for exploratory laparotomy may be forthcoming, it is imperative that the presence of the polyps be confirmed by at least one additional x-ray study.
(b) Small lesions, especially those less than 1 cm. in diameter, may be very difficult to demonstrate.
(c) Furthermore, lesions of any size may be simulated by retained feces and other conditions. The likelihood of errors of this sort is minimized by insistence on at least one repeat x-ray examination.
(d) Stricter preparation for the x-ray examination may be necessary, e.g., liquid or very low residue diet and castor oil early in the evening for two to three days prior to examination.
(e) Even although several polyps may be suspected, definite x-ray confirmation of only a single polyp is required since the presence of a solitary lesion is usually adequate grounds for a recommendation of a laparotomy. Due consideration must be given, of course, to the size and location of the lesion as well as to the age and general medical condition of the patient.
(f) It is impossible to make any definite diagnosis of benign or malignant polyp on the basis of the x-ray appearance alone. All such high-lying lesions must be regarded as potentially malignant. In general, the larger the polyp, the greater the chance of its being malignant.
2. Advise hospitalization and surgical removal of high-lying polyps. (a) This is done because:
(1) About 25% of such lesions will prove to be malignant or exhibit atypical microscopic changes.
(2) The potential for eventual malignant transformation of the other microscopically benign lesions is probably substantial.
(3) In about 25 to 50% of cases the x-ray-detected lesion or lesions will be found to be accompanied by additional unsuspected polyps when the bowel mucosa is inspected at operation. These should also be removed, (b) At the time of operation the surgeon may elect to visualize the mucosa of the entire colon by means of a sigmoidoscope inserted through three small incisions in the bowel (Fig. 74). This procedure is known as colotomy and coloscopy. All lesions found can be removed.

Fig. 74. Colotomy and coloscopy. (After M. R. Deddish.).
3. Re-examine the patient with the sigmoidoscope at six-month intervals for one to two years and then annually.
4. Repeat the barium enema with air contrast study every two years.
If a patient is suspected of having cancer of the rectum and/or colon as a result of symptoms:
1. The management of such a cancer suspect does not differ fundamentally from that outlined previously. Obviously it should include:
(a) Examination of the abdomen and node-bearing areas (for liver and nodal metastasis)
(b) Pelvic examination of women (for local invasion and metastasis)
(c) Guaiac test (for occult blood in stool) and hemoglobin or hematocrit determination (for anemia)
(d) Digital examination of rectum
(e) Sigmoidoscopy
(f) Flat film of the abdomen (if intestinal obstruction a possibility)
(g) Barium enema x-ray with air contrast studies
(h) Chest x-ray film (for pulmonary metastasis)
(i) X-ray of bone on indication (for bone metastasis or invasion) (j) Intravenous pyelogram (for urinary tract obstruction)
2. Biopsy all suspicious lesions and submit material for pathologic examination. If the tissue diagnosis is at variance with the clinical suspicion, do not hesitate to biopsy again from another and possibly more representative portion of the lesion.
3. If barium enema is negative, do not hesitate to repeat x-ray studies one or more times if clinical suspicions persist.
(a) Colon x-ray diagnosis requires great experience and exacting preparation and technique. Nevertheless, lesions may be missed.
(b) The relative blind spots for x-ray diagnosis are:
(1) The rectum
(2) The cecum, especially the posterior wall
(3) The hepatic and splenic flexures
(c) It is worth emphasizing that x-ray examination is notoriously unreliable in the diagnosis of rectal lesions. Yet not uncommonly physicians order a barium enema without doing proctosigmoidoscopy-or sometimes even digital examination. Digital and proctoscopic examination should always take precedence over x-ray whenever a rectal lesion is suspected.
4. If there is reason to suspect low bowel obstruction of any degree, some modification may be required in the routine instruction for bowel preparation prior to sigmoidoscopy and x-ray study, especially with regard to purgation. Otherwise it is possible to accentuate the severity of the obstruction or, at least, give the patient some very uncomfortable hours. Standard measures to rule out obstruction (e.g., flat film of the abdomen ) should be done first if there is any question.
5. The presence of benign disease (e.g., hemorrhoids, diverticulitis, fissures, etc.) that could account for many or all of the presenting symptoms and signs should not deter one from a painstaking investigation to rule out cancer. A distressing percentage of cancer patients have been treated fruitlessly and erroneously in the belief that their rectal bleeding was due to obvious hemorrhoids or that their lower abdominal complaints were merely an exacerbation of long-standing "colitis" or "diverticulitis," etc. Cancer and these common conditions often co-exist. It is the cancer which must be diagnosed and treated.
6. Cytologic examination of washings obtained from the rectum and colon may allow a positive diagnosis in certain problem cases (e.g., diverticulitis vs. cancer) inaccessible to the sigmoidoscope. The procedure is not so complicated as one might suspect, and its accuracy is surprisingly high. A negative report, of course, by no means rules out the diagnosis. Technique for obtaining rectal and colonic washings:
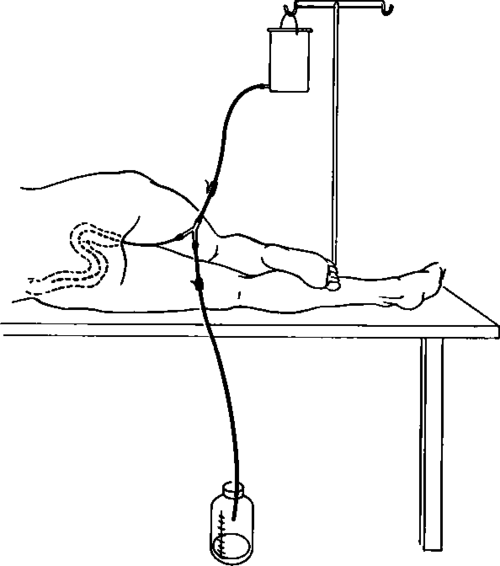
Fig. 75. Setup for obtaining rectal and colonic washings for cytologic study. (For technique, see text.).
(a) Instruct the patient to take 2 ounces of castor oil the afternoon prior to examination and to take tap water enemas until the return is clear on the morning of examination.
(b) Instruct the patient to lie on his left side with the right knee bent. Insert a #18 multi-lumened soft rubber catheter (Fig. 75).
(c) Slowly administer 800 to 1000 ml. of saline solution. After ten minutes collect the return by gravity drainage. The residuum is evacuated by the patient. If the return contains any fecal material, discard and repeat the test.
(d) Measure the return and add an equal amount of 95% alcohol.
(e) As soon as possible, place the specimen in centrifuge tubes and follow the same procedure of centrifuging the specimen and preparing and fixing the slides as outlined for gastric cytology specimens on p. 191.
7. Occasionally the need for exploratory laparotomy may be suggested by clinical indications even in the face of unimpressive x-ray and other evidence.
Continue to:
My Books

