Modified From Georges Laurens
Description
This section is from the book "Applied Anatomy: The Construction Of The Human Body", by Gwilym G. Davis. Also available from Amazon: Applied anatomy: The construction of the human body.
Modified From Georges Laurens
Operations On The Middle Ear
The operations on the middle ear, besides those involving the membrane, are done either for the removal of the remains of the membrane and ossicles, or else to clear out the antrum and mastoid cells and even, if necessary, examine the lateral sinus and jugular vein and explore the brain. They are done for suppurative affections, which may be either chronic, producing local symptoms, or acute, producing in addition constitutional disturbances and even general infection. Caries of the bones is a prominent condition in suppurative cases of long standing, and the character of the operation is dependent on the extent to which the disease has progressed.
In removal of the ossicles, the tympanic membrane is first separated around its edges. Then the tendon of the tensor tympani muscle is cut, and the incus disarticulated from the stapes. The latter is done by cutting with a bent knife across the axis of the stapes and not of the incus (see Fig. 105). The malleus is seized and drawn first down and then out, bringing the membrane with it, and afterwards the incus, which is detached by Ludwig's hook (see Fig. 106), is removed, and, if desired, the stapes. Granulations and pus are removed by the snare, forceps or curette. Care is to be taken to avoid, if possible, scraping away the thin shell of bone on the internal wall that covers the facial nerve. Any twitching of the muscles of the face indicates that the nerve is being irritated. The chorda tympani nerve, which passes on the inner side of the handle of the malleus and lies beneath the mucous membrane, is of necessity removed. No important symptoms follow its removal.
Operations On The Antrum And Mastoid Cells
In order to understand these operations, one must recall that the suprameatal crest is the ridge of bone forming the upper edge of the bony meatus, and a continuation backward of the posterior root of the zygoma. The upper and posterior edge of the meatus is formed by a thin, small shell or edge of bone running from the suprameatal crest downward and backward to the posterior wall; this is the suprameatal spine. Behind the suprameatal spine and between it and the posterior portion of the suprameatal crest is a depression, the suprameatal fossa. This suprameatal fossa is triangular in shape. The crest forms the upper side, the spine its anterior side, and the ridge of bone, running from the posterior portion of the crest to the lower portion of the spine, forms the posterior side. These three lines form the suprameatal triangle of Macewen. It is through this triangle that the antrum may be reached. The operation may be restricted to the antrum and tympanic cavity, or may include the whole or part of the mastoid cells, constituting the operation known as tympanomastoid exenteration.
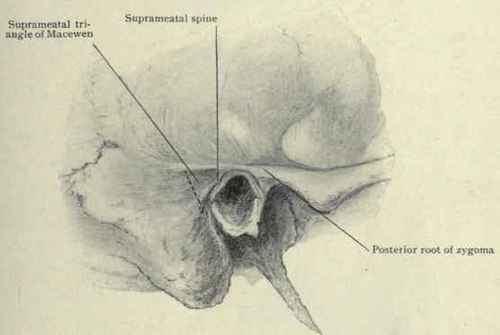
Fig. 107. - Landmarks for operating to enter the mastoid antrum.
To reach the antrum a semicircular cut is made a centimetre back of the ear and the ear and membranous canal loosened and pushed forward. With a gouge chips of bone are removed from the suprameatal spine backward and from the crest downward as far as desired. This will extend considerably beyond the line marking the posterior boundary of Macewen's triangle. The outer table of bone being removed, the cells are broken through parallel to the meatus and slightly upward, for the lower level of the antrum corresponds to the upper edge of the meatus. It is hardly safe to penetrate deeper than 1.5 cm. (3/5 in.) from the meatal spine inward, for fear of wounding the facial nerve. The mastoid antrum lies not only above and posterior to the membrane and tympanic cavity, but extends outward along the posterior and upper portion of the canal, and the facial nerve can be wounded only by passing across the antrum and attacking the bony covering of the Fallopian canal below and anteriorly.

Fig. 108. - The mastoid antrum exposed by chiselling through the suprameatal triangle. The mastoid cells exposed by chiselling off the surface of the mastoid process.
In doing a tympanomastoid exenteration, a more extensive procedure is performed. It consists in cleaning out the various communicating cavities and throwing them together, thus making their interior more accessible. The antrum is reached in one of two ways: either posteriorly, or anteriorly through the meatus. The posterior operation, or that of Schwartze, Zaufal, and others, consists in removing the membranous lining of the bony meatus on its upper and posterior portions down to the tympanic membrane. The antrum is then entered as already described; the posterior bony wall of the meatus is chiselled away, giving access to the tympanum; the ridge of bone separating the roof of the bony meatus from the attic or epitym-panum is chiselled away (see Fig. 109), and the membrane and ossicles removed. This gives access to the tympanic cavity, epitym-panum, and antrum. As much of the mastoid cells as necessary is exposed by chiselling away their external covering of bone even down to the tip of the mastoid process.
If the anterior operation of Stacke is performed, the membranous lining of the bony meatus is to be loosened and divided as close to the membrane as possible and drawn forward with the cartilaginous meatus. The drum membrane and as much of the ossicles as possible are then to be removed, and with a chisel or bent gouge the angle, or ridge of bone between the upper side of the bony meatus and epitympanum, or attic, cut away. The antrum is now entered by chiselling away the upper posterior wall and the chiselling away of bone continued until the mastoid cells have been sufficiently exposed. The final result of these two methods is the same. The external meatus, tympanum, epitympanum, antrum, and mastoid cells are all thrown into one large cavity. Wounding of the facial nerve is to be avoided by first learning its course and then by sponging away the blood and cutting only the structures which are clearly visible. Tracing the facial nerve backward, it is seen (Fig. 103) entering the stylomastoid foramen, passing upward posterior to the tympanic cavity, and crossing at about its upper edge to pass above the oval window. Viewed in Fig. 101, it is seen that the Fallopian canal lies a trifle nearer to the external surface than does the tympanic membrane, so that in making the opening into the antrum or in connecting the mastoid cells below the antrum with the tympanic cavity, care should be taken to keep a little anterior or superficial to the membrane.

Fig. 109. - Chiselling away the spur of bone between the roof of the external auditory meatus and attic or epitympanum.

Fig. 110. - Lateral view of the temporal bone, showing the relations of the lateral or transverse sinus and mastoid antrum.
Continue to:
My Books

