The Female Perineum
Description
This section is from the book "Applied Anatomy: The Construction Of The Human Body", by Gwilym G. Davis. Also available from Amazon: Applied anatomy: The construction of the human body.
The Female Perineum
The perineum in the female is much like that of the male. It has a central point at which converge the external sphincter ani from behind, the superficial transverse perinei muscles from each side and the bulbocavernosus muscles from the front. The ischiocavernosus muscles lie along the rami of the pubes. These superficial muscles are reinforced by the deep transverse perinei muscle, which comes from the ramus of the ischium on the side to insert by its anterior fibres around the urethra (compressor urethrae), its middle fibres into the vaginal wall, and its posterior fibres at the central point of the perineum. Also the levator ani muscle inserts into the lower end of the vagina anteriorly, then into the central point of the perineum, next into the lower end of the rectum, and finally into the coccyx. The deep layer of the superficial fascia (Colles's fascia) and the triangular ligament being pierced by the vagina are not so marked as in the male - between them lie the ischiocavernosus, bulbocavernosus, and superficial transverse perinei muscles (Fig. 467).
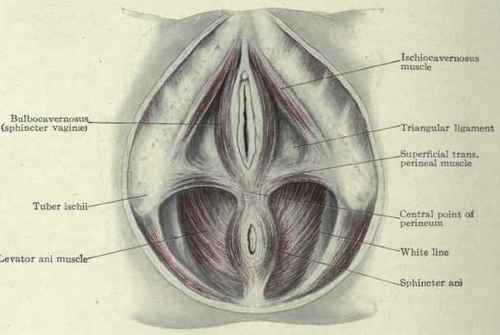
Fig. 467. - Female perineum.
Rupture Or Laceration Of The Perineum
When the tear goes only part way through the perineum it is called an incomplete laceration; when it goes through into the rectum it is a complete tear.
In an incomplete tear the bulbocavernosus muscles (called also sphincter vaginae) are separated behind and consequently their function of holding the labia majora together is lost and the vulva gapes. In a complete tear all the muscles helping to form the perineum are divided: they are the bulbocavernosus, the superficial and deep transverse perinei, and the levator ani and external sphincter ani muscles. They draw the sides of the wound apart, sometimes forming a dimple on each side, and thus enlarge the vaginal outlet and allow the anterior wall of the rectum as well as the posterior wall of the bladder to prolapse (Fig. 468).
Operation
The torn area is to be denuded by beginning the incision not higher up than the lower end of the labium minus on one side and carrying it down and then up to a corresponding point on the opposite side. From the extremities of this incision two more are made extending 2.5 to 5 cm. (1 to 2 in.) up the vagina and meeting in the median line. Emmet carried the denudation up each lateral sulcus. The mucous membrane so marked out is then dissected away; to close the wound some operators introduce and bring out the stitches all on the skin surface, while others introduce and tie half of them on the vaginal surface and the other half on the skin surface. The needle is to be carried well out toward the rami of the ischium so as to include a large mass of tissue.
If the mucous membrane of the rectum has been torn it is to be sewed together before the perineal tissues are approximated.

Fig. 468. - Rupture of the perineum. The vulva gapes, showing the rectum bulging forward; the two dimples, one on each side of the anus, are caused by the retracted muscles.
Continue to:
My Books

