Treatment Of Deep-Seated And Tuberous Naevus
Description
This section is from the book "A Treatise On The Materia Medica And Therapeutics Of The Skin", by Henry G. Piffard. Also available from Amazon: A Treatise On The Materia Medica And Therapeutics Of The Skin.
Treatment Of Deep-Seated And Tuberous Naevus
This requires, as a rule, quite a different course of procedure from those just noticed. The various methods that have from time to time been recommended are almost too numerous to mention, and the choice between them is to be guided in part by the results attainable, and in part by the size, location, or other peculiarities of the individual case under notice. The comparative safety or danger of the different operations is also to be taken into consideration. These are matters that specially call for the exercise of good judgment on the part of the surgeon. For the treatment of smaller naevi, that is up to one or two centimetres in diameter, a number of procedures are applicable.

Fig. 18. - The author's cutipunctor.
First
The tumor may be injected with a coagulating fluid, as one of the salts of iron. This has been frequently successful, but it is not devoid of danger, as coagula have been carried into the circulation, and fatal embolism has resulted.
Second
Fluid extract of ergot may be injected (Hammond) with a view to inducing contraction and diminution of the calibre of the vessels.
Third
Setons may be introduced for the purpose of exciting adhe-sive inflammation.
Fourth
In an unvaccinated person the insertion of the cow-pox virus has excited sufficient inflammation to obliterate the growth.
Fifth
Electrolysis may be employed. This, as is well known, consists in the introduction of properly insulated needles connected with a galvanic battery. The best material for the needles is irido-platinum; the one connected with the positive pole should certainly be made of this or of some other hard non-oxidizable metal. The negative needle may be gilded steel. Some writers recommend that the positive needle alone, others that the negative needle only, be introduced into the tumor, the circuit being closed with a sponge-covered electrode connected with the other pole and applied to the neighborhood of the naevus. Personally I prefer to introduce both the positive and negative needles at the same time into the tumor. It must be recollected, however, that the effects produced by the different needles is not the same. The positive needle causes coagulation of the albuminous fluid in immediate contact with it, and a small tubular, somewhat adherent clot, forms immediately around it. At the negative needle no coagulation is effected, but rather the contrary - that is, decomposition (true electrolysis) of the surrounding fluid with destruction of the tissues. After the galvanic current has passed for a suitable time, the needles are withdrawn. The negative needle comes out readily, but the positive sticks a little and will require a little force for its withdrawal. It is better not to use this force, but for a moment before withdrawal to reverse the direction of the current, which changes the former positive needle into a negative one, and permits its ready extraction.
Sixth
The actual cautery may be used. I well remember the first time I saw this method employed, nearly twenty years ago, at the hands of my preceptor, Prof. Willard Parker. The instrument used was a common shoemaker's awl, heated in the flame of a spirit-lamp. This, brought to a dull red heat, was several times plunged into the tumor. A somewhat better instrument is provided with a solid metallic globe, as shown in the annexed cut, Fig. 19.

Fig. 19. - Small cauterizer.
The globe serves as a reservoir of heat, and permits the operation to be performed with more deliberation, and even allows several punctures to be made without reheating. The galvano-cautery may be used instead, but is not equal in convenience to a fine pointed Paquelin cautery (Fig. 20). The point which I usually employ is of the form and size here shown. The point should not be brought to a white or even a bright red heat, as hemorrhage would be likely to follow its introduction. It is better, having heated it to a red heat, to let it cool until the color is just about to vanish and then introduce it. A few puffs on the rubber bulb of the instrument preserves the heat in readiness for the next puncture.
Seventh
The naevus may be excised, as particularly recommended by Dr. George Buchanan (116, 1/75, 831).
Eighth
The tumor may be ligated. The ordinary methods of lighting naevi are fully considered in most works on surgery, and to these I must refer the reader for details as to the operation. A modification of the ordinary ligature operation has been recently devised by Mr. Richard Barwell, and is described as follows (137, May 8, '75):

Fig. 20. - Fine point belonging to the Paquelin cautery.
"Having carefully made out the limits of the naevus, both as to its depth and circumference, a needle, armed with not too fine a wire, is passed through the skin half round the tumor, and out again opposite the place of entrance; the needle is then again introduced at the same puncture by which it had just emerged, and, passing round the other side of the tumor, makes its final exit at the opening first made.
"In certain cases, large size or peculiar shape of the tumor may render it necessary to bring out the needle twice instead of only once. However that may be, the effect is to enclose the base of the tumor in a wire loop, both ends of which, emerging at the same opening, are under perfect control. These might merely be twisted together till the requisite tightness is attained, but in this practice certain inconveniences arise, which I have obviated by another expedient. A vulcanite oval plate, about three-fourths of an inch long and an eighth of an inch thick, has two holes bored obliquely through its thickness; and on its external surface two little studs project close to where these holes emerge, and where, also, they are farthest apart (Fig. 21).
"By bringing the end which passes by the right side of the naevus through the left hole, and vice versat the wire is made to cross, while the oblique direction of the holes permit it to run smoothly. The surgeon having thus arranged his appliance, draws upon the wires until the naevus is rather tense, and then twists each end round the nearest stud. A piece of lint, slit so as to bestride the wire, is introduced between the skin and the vulcanite button, and prevents any undue pressure by the edges of the plate.
"On the third or fourth day the wire will have become somewhat loosened; one of the ends is to be untwisted from the stud, drawn tight, Of the various methods for the treatment of Naevus, it must be remembered that while all have yielded good results, all have sometimes proved disappointing even at the hands of skilful surgeons.
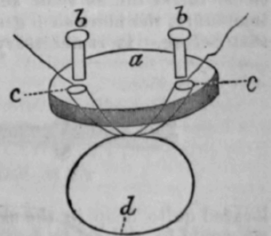
Fig. 21. - a, vulcanite disk; ft, brass studs; c, holes pierced obliquely in direction of dotted lines; d, wire looped as in and again secured. This process is to be repeated until the wire comes away, when, as must be evident, it has not merely strangulated, but has cut through the base of the naevus with all its vessels of supply; in fact, it has acted as a slow but sure ecraseur."
Continue to:
My Books

