Lecture XV. Duodenal Alimentation
Description
This section is from the book "Lectures On Dietetics", by Max Einhorn. Also available from Amazon: Lectures on Dietetics.
Lecture XV. Duodenal Alimentation
Duodenal alimentation means feeding a patient through the duodenum in such a manner that the stomach is kept empty. This can be done by introducing a small tube into the the stomach, whence it passes of itself into the duodenum, and is left there. The main purpose of this method is that we should have the patient always ready for feeding, independent of his desire to eat or his aversion to food. It is easily done. The tube can even be allowed to go into the small intestine, depending upon the length of the tube.
I have practiced this method for the last ten years and have treated 500 patients by this method, for periods varying from ten to fifteen days - most of them from fourteen to fifteen days.
The food is usually given every two hours, eight feedings a day. The standard food is milk (7 to 8 ounces), one egg, and a tablespoon-ful of lactose. The lactose sometimes causes diarrhea and should then be omitted. In some cases where it is essential to see that there is no loss of flesh, butter (1 to 2 drams) and also barley flour may be added in every alternate or in each feeding. This standard diet furnishes 2215 calories. If in addition, one ounce of lactose is given, it brings it up to about 2695 calories for a grown person. If butter is added, it brings it up to 3000 and more calories. Only a few patients cannot stand the milk, the latter creating such a disturbance that it must be eliminated. Such patients tell you that they never could take milk anyway. Here instead of milk, water with barley or pea flour can be substituted or vegetable milk employed. Whatever is fed to the patient must be of blood temperature - neither cold nor hot - strained over a cloth, and it must be given slowly. When I began to feed these patients I made use of an irrigator, letting the fluid run in by gravity which would carry it to the duodenum, but it was soon found that this was very inconvenient. The temperature cannot be so well maintained, and the flow is either too quick or too slow. It was very troublesome, and the patients could not stand it, so a syringe was devised, provided with a three-way stopcock and with a little table (Fig. 6), so that there is no need of loosening the syringe from the tube each time the former has to be filled, and the feeding can be made slow or fast as desired. The patients usually prefer to have it administered slowly, for if given quickly they feel uncomfortable. It is a very tedious performance, but the patients can soon learn to feed themselves, and it gives them something to occupy themselves with. It requires about twenty minutes or so for each feeding, and that repeated for eight times a day, gives them something to do.
1 Delivered before the Clinical Society of the New York Post-Graduate Medical School and Hospital, March 21, 1913, and published in the Postgraduate, June, 1913.

Fig. 6. - The duodenal feeding apparatus, with table support. A, tube leading to syringe; B, tube leading to duodenal pump; C, crank; D, tube leading to fluid; F, fluid; G, glass; T, table support or shorter support. When crank C is turned parallel to A, fluid can be aspirated from the glass into the syringe. When C is moved parallel to B, the fluid from the syringe can be emptied into the duodenum.
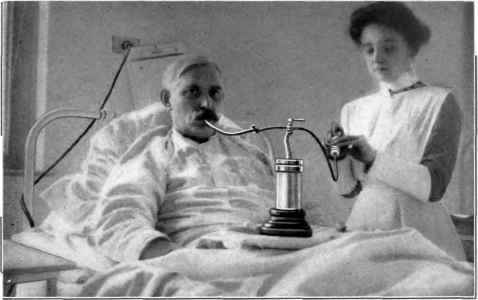
Fig. 5. - Patient being fed through the duodenal tube.
Instead of using the syringe all this time for the injection of the entire amount of nutriment, this can be advantageously arranged after Burkhardt by syphonage. Proceed as follows: Turn crank to A and fill up the syringe, then turn crank to B. and inject about 4/5 of the syringe into the duodenum. Turn crank midway between A. and B. parallel to the tube connecting the table with the nutriment in the container and leave it this way. The fluid after having been primed continues to run steadily by syphonage - should the flow stop, the syringe is filled up again and the process repeated as described.
This way of feeding is more agreeable to the patient and less laborious.
A word in regard to the technical points of this method of alimentation. The tube is put into the throat of the patient and he swallows it with water. Care must be exercised that the patient does not swallow it too quickly, so that it does not rotate on itself, but will be taken straight into the stomach. Then, a little later, liquid food is given by the mouth and tests are made from time to time through a syringe attached to the tube to see what can be obtained. If the duodenal tube is still in the stomach an acid liquid appears quite quickly by aspiration. If the tube is beyond the pylorus, in the duodenum, it is very difficult to obtain fluid, for the duodenum is usually empty. The secretion appears slowly in drops from time to time and shows an alkaline reaction. Another point of differentiation is that if we should put in air through the syringe, the patient feels it right away if the pump or tube is in the stomach; but if the tube end is in the duodenum there is less conscious sensitiveness and the patient does not feel the air at all. If we have to deal with a patient who has no gastric secretion it is more difficult to determine when the pump has entered the duodenum. Here there is no acid in the stomach anyway, and in order to ascertain whether the pump is in the stomach or duodenum, we make use of different colored fluids. For instance, a patient who has had no milk, but only bouillon or tea, may be given a white (colored) fluid, such as milk. If we then aspirate and obtain a fluid that is not white, we known that the tube end is beyond the stomach. If the patient had milk we give him black coffee, or any colored fluid that is not white.

Fig. 7. - Patient L. K. with duodenal tube in the duodenum with empty stomach. The X-ray photographs (Figs. 7 and 8) were kindly made for me by Dr. W. R. Stewart, Radiologist to the Lenox Hill Hospital.
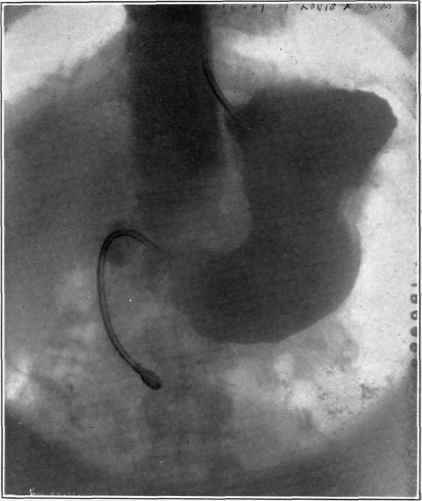
Fig. 8. - Patient L. K. after the ingestion of a bismuth mixture into the stomach. The end of the duodenal tube is distinctly visible outside of the stomach, in the duodenum.
Continue to:
My Books

