Massage As A Remedy In The Treatment Of The Wounded. Continued
Description
This section is from the book "Massage Its Principles And Practice", by James B. Mennell. Also available from Amazon: Massage It's Principles and Practice.
Massage As A Remedy In The Treatment Of The Wounded. Continued
Volumes could be written on the subject - "Tommy: A psychical study." The outlook on life varies between the two following examples. " ' Eart-breaking work for you, sister, ain't it, trying to get us fellows well, when none of us mean to be fit again till the war is over!" represents one extreme of thought; while the other limit was reached by the man who, having been on the top of the Vimy ridge for months, was invalided home as "G. S. W. femur, septic." In spite of two inches shortening and two plugs, so great was his desire to be with "the boys" when they charged down the slope of the ridge, that, hoping to hasten his recovery, he refractured his femur by abuse of freedom when first allowed out of ted.
"Shell-shock" is a phrase that has caught the public eye as something quite new. The only novelty about it is perhaps that, as Farquhar Buzzard has pointed out,1 it is rare to find in the whole realm of medicine and surgery any term that covers such a multitude of various conditions - unless, indeed, it is "railway-spine." Grouped together under this heading we find every variety of case from the pure malingerer to cases of severe head or spinal injuries - from the insane to the man who was "fed up" and wanted a week or so in "Blighty."
Buzzard classes "shell-shock" cases more or less into the following groups : -
First, "cases of pure exhaustion" - i.e., men whose natural reserve of nervous energy is limited, and who therefore soon show symptoms of the lowering of the amount of nervous potential that is available for the use of the organism. These patients are pure neurasthenics and should be treated as such.
The second class contains those "who have inherited neuropathic or psychopathic tendencies, and in whom the process of exhaustion has excited these dormant tendencies into activity." This is simply expressing in other words the fact that psychasthenic soil is a fertile one on which the plant of neurasthenia flourishes. They require treatment as for neurasthenia, until this element of the combined disorder has been obliterated. The psychasthenic element can, of course, only be dealt with adequately by psychical treatment.
1 Lancet, December 30, 1916.
The third group is described as consisting of "martial misfits," and consists of a limited number of men who, by temperament, training, or both, are totally unfit for military duty. They undertake the duty with this knowledge, realising all the time that the road they are treading leads to inevitable "smash." When this arrives they are simply victims of neurasthenia, the fatigue in this instance being due in the main to the incessant outrage inflicted on the unconscious mind via the conscious.
The fourth group consists of men who have suffered actual concussion. Recovery may be apparently rapid, but in reality no one ever makes "rapid" progress after any severe head injury. It always leaves its echo, as it were, behind; and unless sufficient rest is enforced (Buzzard puts it at four weeks in bed at least), the patient almost invariably exhibits some signs of neurasthenia.
The fifth group, unfortunately not a small one, comprises cases which are dubbed as "shell-shock," but which in reality are suffering from some organic (and not psychical) lesion of the central nervous system. Each calls for treatment suitable to the symptoms produced by the lesion.
The sixth group consists of hysterical cases, "who suffer from so-called functional paralysis, anaethesia, mutism, aphonia, deafness, blindness, etc." Reference to the chapter on Neurasthenia will show that massage treatment is not extolled as a remedy for these cases. They are not malingerers; they are men whose personal consciousness has contracted. They therefore require psychical treatment, not physical.
The seventh group consists of malingerers pure and simple. Of these Buzzard says, "My belief in the general honesty of the human mind leads me to the conclusion that such persons are extremely rare." Many surgeons will dissent from this opinion, but the physician is the more competent judge of this type of case. Massage for the malingerer is obviously waste of time.
When "shell-shock" is thus reduced to its component parts it becomes evident that this is no new disease created by warfare. Given accuracy in diagnosis, we are only confronted with conditions with which we are quite familiar decked out under a new title. Perhaps it is as well, for it is preferable that the public should regard most of these poor fellows as "shell-shock" cases rather than as "suffering from hysteria and neurasthenia. But this analysis of "shell-shock" cases serves once more to emphasise that we should as a rule extend to the victims of neurasthenia not only our sympathy, but also our admiration for the magnificent fight put up, with insufficient strength against overwhelming odds, before they are finally crushed.
As the result of war injuries we are called upon to deal with a very large number of amputation cases. There is nothing particularly new about their treatment; each case has to be considered on its merits and dealt with accordingly.
In one type, the scar is adherent and requires loosening. In another, some nerve is caught in the scar and requires to be shaken loose. If pain is due to a bulbous end, vibrations may suffice to cure, as also if the nerve is bound down by adhesions.
We may only require to restore nutrition; but usually, whatever else there may be to do, some structures will need stretching. Whenever this is so, the case should be dealt with by gradual tension of the contracted structures while kneading, shaking, or vibration is performed. It is a tedious and tiring job, as considerable physical strength is required, and progress is seldom rapid. It is frequently possible to hasten it, however, by the prescription of suitable exercises. There are few of these cases for which some form of active exercise cannot be devised - in addition to the administration of assistive and resistive exercises. In one type, however, this is practically impossible, namely, after amputation through the upper third of the thigh. These cases are very difficult to deal with, when the problem is to restore extension and adduction. The strain on the masseur's wrists is very great, as the effort required varies in direct proportion with the shortness of the stump. It is almost essential for two people to work together: one holds the thigh of the sound limb fully flexed upon the abdomen so as to immobilise the pelvis, while the other performs the manipulations. So great is the strain, and so much physical exertion has to be expended, that very few cases can be dealt with daily by any pair of masseurs.
To overcome the difficulty we have given trial to many devices at the Special Surgical Hospital at Shepherd's Bush. At last we have hit on a plan which bids fair to yield success. My two masseurs, Sergeant-Major Pavitt and the blind masseur, the late Mr. N. Webb, first gave it trial. It has proved most successful, and they, with our carpenter, A. J. Hobbs, have made a notable advance in our treatment of these very difficult cases.
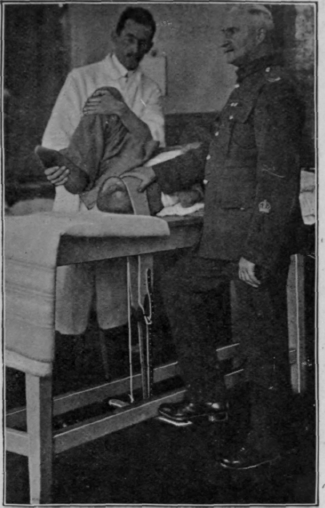
Fig. 167. - The table and apparatus in use at the Special Surgical Hospital for stretching thigh amputation cases with flexion deformity.
Two parallel slits are cut in the top of the massage-plinth, and through these a horse-girth is passed which surrounds the stump. The ends of the girth are attached to a lever which can be depressed by the foot. This is also controlled by a spring. One masseur then flexes the sound thigh to its full extent, while the other exerts tension on the stump by pressing down the lever with his foot. Both his hands are thus free to knead the tightened structures. The adduction is secured manually, and also by altering the position of the patient's pelvis and by lateral pressure (see Fig. 167 and Appendix). The use of this table can be extended to many other conditions, and notably to that in which full extension of the knee is restricted. During the application of the tension the patient should use his own muscles as far as possible in order to assist in securing the movement desired.
Throughout the pages of this book repeated reference has been made to the use of "exercises," and it has been said that nothing can replace the ordinary use of a limb as a remedial agent. No reference to treatment by exercises can therefore be considered complete unless it includes work done in the remedial workshops now arranged in connection with many of the hospitals for the wounded. Here the remedial agent is productive work which entails general use. Thus not only are muscular strength and co-ordination re-developed, but the psychical effect on the patient is of the greatest value. The work referred to is designed for the restoration of function and is quite distinct from occupational re-education, which, however, is no less important to many of the disabled. To H.M. King Manuel our wounded owe a debt of gratitude for his ceaseless labour in this branch of remedial work, which he has made so specially his own.
Continue to:
My Books

