Recent Injury Treatment By Mobilisation And Massage. Part 2
Description
This section is from the book "Massage Its Principles And Practice", by James B. Mennell. Also available from Amazon: Massage It's Principles and Practice.
Recent Injury Treatment By Mobilisation And Massage. Part 2
Various explanations have been advanced as to the pathology of oedema after injury in the absence of sepsis. Local effusion may add to the general swelling: it does not cause it. The venous return is deprived of the assistance normally rendered by muscular contraction, but this cannot suffice to account for an intense oedema which may make its appearance in the course of a few hours. Mechanical obstruction to venous or lymphatic return might play its part in a few selected cases where fracture or dislocation has caused pressure on a main venous trunk, but the swelling may be very acute even if this possible source of trouble is wanting. Ill-applied bandages or splints will, of course, greatly aggravate the swelling by supplying the obstruction which the injury has failed to provide.
There remains one more explanation - reflex disturbance of the vaso-motor mechanism. There is evidence that this is the true cause of most of the swelling. If we consider the oedema following all fractures through the lowest inch of the radius, it will be found that, given equal severity of injury, it will be greatest in elderly or decrepit patients, least in children, and varying in severity according to age throughout the intervening periods of life. For this phenomenon there is no other explanation than that it is due to vaso-motor disturbance, which is prolonged in the aged, transitory in children, and of a duration which varies directly with the so-called "powers of recuperation" at various ages.
We are left, then, to devise a treatment for definite injuries to certain structures, and for a disorganised circulation.
Obviously we cannot heal torn fibres by massage, but we can assist in restoring the circulation on which the repair depends, and not only the repair of these fibres, but of all the various injuries that have been sustained.
Keeping in mind that the circulatory system is the curative agent, and that this has suffered reflex disorganisation, it becomes apparent that the first duty of the masseur is to counteract this inimical reflex if possible. This can be accomplished in one way only, namely, by sending up to the nerve centres stimuli calculated to procure what might be called, in contra-distinction, a beneficent reflex. In massage we have an agent that can directly assist in procuring this reflex, and in massage alone. The technique that should be followed will be clear from what has been said in the preceding chapters.
The first duty is to send up to the posterior nerve roots stimuli which will procure a reflex to counteract the stimuli from the injury. This is done by slow, gentle, rhythmical stroking of the surface of the limb. From hand to elbow may suffice, but it is often necessary to make a long, straight, steady sweep from wrist to shoulder, or vice versa. The arm must be hanging comfortably by the side with the forearm and hand firmly supported.
It is, perhaps, not fully realised what is the origin of the spasm or cramp after fracture. The explanation of the phenomenon is simple. After fracture there is a reflex attempt on the part of the muscles to check any wider displacement of the fragments, and so prevent any further damage from being done by their movement. It follows, therefore, that spasm is least noticeable when mobility of the fragments is least, and greatest when they are freely mobile. Thus we find that it is least in greenstick and fissure fractures, and greatest when there is great displacement. Further proof is seen when sensation is lacking in a tabetic patient. Though the fragments may be freely mobile their movement does not convey to the central nervous system the call for protective spasm, as the paths along which the call must travel are blocked by disease. Hence the lack of spasm, which, as explained elsewhere, accounts for the lack of pain.
It is plain then that, if we wish to relieve spasm, postural treatment is of paramount importance. No relief can be secured, no relaxation can take place, if the posture is such that, on the cessation of the spasm, the fragments will tend to move in any direction other than that which entails their restoration to their original position. The first requisite, therefore, in dealing with any case of cramp or spasm is so to arrange the posture of the patient that, on the relaxation of the muscles taking place, no condition is present that would cause them again to pass into reflex protective contraction.
A few minutes after the treatment is begun, provided the postural treatment has been duly respected, the patient will begin to feel the pain "easing off," and the masseur notices that the forearm no longer presents the brick-like resistance to the hand as it passes along. A few minutes later the forearm will become as soft as the arm, and the patient will experience great relief.
It is probable that some involuntary relaxation of the fingers will be noticed as the spasm passes off. The first indication which the masseur will be able to note is the general softening of the forearm muscles. As soon as the latter are quite soft it will be found that the fingers are no longer maintained rigidly fixed, and the support that they have hitherto received may be slowly and alternately withdrawn and replaced. This will impart a slight movement, which will gradually increase in amplitude. As soon as they are capable of relaxed movement through a perceptible range, the support of the hand may be so altered as to allow a slight dropping of the wrist and return to its former position. The movement, imperceptible at first, gradually increases, when a small degree of rotation may be added by slightly altering the position in which the support is re-adjusted. It is now possible to administer flexion of the wrist with supination, and extension up to the original position with returning pronation.
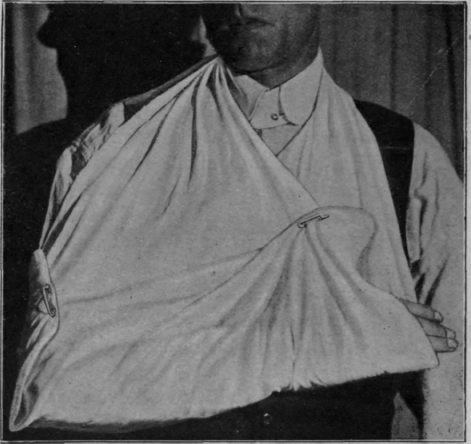
Fig. 63. - Correct position for carrying the forearm in a sling.
Continue to:
My Books

