Sprains and Dislocations Treatment. Part 3
Description
This section is from the book "Massage Its Principles And Practice", by James B. Mennell. Also available from Amazon: Massage It's Principles and Practice.
Sprains and Dislocations Treatment. Part 3
Dislocation of the wrist or of any individual bone of the carpus is always a severe injury. If the wrist has suffered, all that has been said on the subject of fracture through the lowest inch of the radius holds good as indicating the line of treatment to be followed. It is not a common injury, and, after reduction, the surgeon will probably have placed the wrist in a slightly dorsi-flexed position. If so, the formation of disabling adhesions is not likely to occur (Robert Jones) and restoration of function should be rapid.
If one or more bones of the carpus have been dislocated, open operation is almost essential to success. If a tentative trial is to be made to see whether massage and mobilisation can effect a cure, treatment should aim at restoring dorsi-flexion. This law should be respected in the massage-room as well as in the operating theatre during the treatment of all injuries of wrist and carpus below the level of the lower end of the radius. If this position is not secured, and if the dislocation is left unreduced, months of massage and manipulation will probably effect only a very partial restoration of function. Any attempt to hasten the process will render it more prolonged. Otherwise treatment may proceed on the general lines mapped out for Colles' fracture (see p. 157). If any offending fragment has been removed by operation, treatment is the same, but much more rapid progress can be made. Again dorsi-flexion must be maintained.
A detailed account has been given (p. 129) of treatment applicable to fracture without displacement through the lowest inch of the radius. This will furnish a full guide for treatment of a sprained wrist. Most severe "sprains" in this situation will be discovered to be fissure fractures on examination with the X-rays, the most common being a fissure fracture through the radial styloid process.
All injuries in the hand may be treated on general lines. Dislocations are very liable to recurrence, and so active move-ment must be prescribed cautiously. Massage to hasten repair must be applied to the whole limb, or at least to the level of the elbow. All movements of shoulder and elbow should be prescribed freely to encourage circulation and prevent stiffness.
Dislocations of the hip are not very liable to recur in the massage-room. The injury is most severe, and the surgeon invariably prescribes treatment. Recovery would be more rapid as well as more complete were mobilisation started at an early date. The chance of the dislocation recurring as the result of treatment can only be negligible, while delay inevitably entails the formation of adhesions. General massage for reflex effect and for circulation is called for; the patient should be taught to exercise all muscles, and internal rotation is the last movement that should be administered or prescribed.
Sprains of the hip are very rare, as fracture or dislocation takes place instead. If met with they should be treated on general lines.
Dislocations of the knee never arrive in the massage department while the injury is still recent. Sprains, cases of "water on the knee" from various causes, and "slipped cartilage" cases that have been reduced, are frequently recommended for treatment by mobilisation and massage.
In the treatment of all cases of injury to the knee two points must be kept in mind - first, that the injured structure must be guarded from strain while repair takes place, and, second, that the quadriceps extensor will waste as a whole, but that the lower fibres of the vastus internus will do so more rapidly and more thoroughly than the rest of the group. The result of this is that, when the quadriceps contracts as a whole, the patella will be drawn up somewhat obliquely to the natural line of movement. Thus, in Fig. 91, if A is the line of pull of all the muscles except the vastus internus, B is that of the vastus internus, and C the resultant of these two forces, C will represent the normal line of movement of the patella. It is obvious that any diminution of the force B will tend to shift the resultant C nearer to A. In addition the lateral fixation of the knee is insecure, and a certain amount of preternatural mobility is possible. The clinical effect is recurrent effusion. Hence the importance that must always be attached to building up the strength of these fibres of the vastus internus. This may be effected in three ways. During normal extension of the leg the vastus internus contracts in proportion to the other muscles, but in forcible extension it seems to play a more prominent part. Hence the patient should be instructed to "try to bend the knee backwards" both lying and standing. The second exercise is merely a special application of this method, namely, tip-toe walking with knees stiff. The third is performed from the fundamental standing position, the knee is slightly slackened, and an attempt is made to rotate the joint inwards. This requires practice, but is effective. All three are rather monotonous and require persevering repetition. If this is not forthcoming, or if the wasting is marked, treatment by graduated faradic contraction should be given.
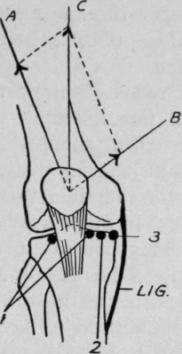
Fig. 91. - (After Robert Jones.) To show how wasting of the vastus internus alters the resultant of the direction of the pull of the whole quadriceps, thus causing the movement of the patella to deviate from its normal direction.
A, line of pull of the quadriceps as a whole.
B, line of pull of the lower fibres of the vastus internus.
C, resultant line of movement of the patella.
1. Tenderness at these points on extension indicates a tender post-patellar pad.
Continue to:
My Books

