The Treatment Of The After-Effects Of Injury. Part 4
Description
This section is from the book "Massage Its Principles And Practice", by James B. Mennell. Also available from Amazon: Massage It's Principles and Practice.
The Treatment Of The After-Effects Of Injury. Part 4
If a joint is stiff, massage may be used as an agent in restoring mobility. The limb is supported in a position which corresponds to that adopted during the administration of relaxed movement, but with the difference that the support is withdrawn from the stiff joint so as to allow a certain amount of strain to fall upon it. Massage is then continued in such a manner as to add slightly to this strain, and each addition of movement is controlled by the other hand. The hand that performs the massage can detect any tendency to spasm on the part of the muscles controlling the movement, and can then deal with it by firm stroking, kneading, or shaking,1 as may seem most desirable. If this does not suffice to secure relaxation, the other hand can release some of the tension. Relaxation can often be secured by calling upon the antagonists actively to contract.
The first step in the movement of a joint, which is not perfectly supple, is to discover, if this is not already known, how much free movement is possible, and how far, owing to anatomical alterations in the part, it may or may not be practicable to restore full movement. The latter information can be gained only from the medical man, as the prognosis depends almost entirely on the knowledge of what has already happened. The administration of a dose of relaxed movement should always precede any attempt forcibly to move a joint, and sub-maximal movement may be repeated with ever-growing amplitude till the limit of free movement is reached. Then should begin slow, steady pressure aided by massage, every bit of "slack," as it is secured by the hand which is performing the massage, being as it were, "taken up" by the hand which is controlling the support. Voluntary effort, however, should always be encouraged. Try as we may, no stiff joint will ever recover unless the patient does his share of the work.
1 For the description of "shaking" see p. 47. It differs somewhat from the Swedish movement described by the same name.
The use of mechanical agencies may also be invoked, as for instance the sliding seat when attempting to add flexion to the knee (see Fig. 50, p. 104). In the same way the weight and pulley apparatus, or the ladder, can be utilised to assist the restoration of almost any movement, both hands of the masseur being then at liberty for massage, or to assist in the movement, as may be most desirable (see Fig. 92). The administration of prolonged traction or pressure will do far more to restore a few extra degrees of flexion than any number of sudden jabs, unless freedom of movement is almost perfect. In this case, namely, when the patient has practically recovered from the point of view of mobility, intermittent pressure may often replace the constant pressure here advocated, but it is a great mistake to allow it to do so in the earlier stages. Almost up to the end of treatment sub-maximal relaxed movements may be repeated, but not the forced movements.
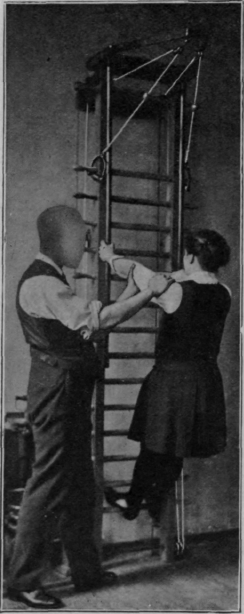
Fig. 92. - To show one method of assisting movement while the patient is exercising on the ladder. The masseur is assisting extension of the elbow.

Fig. 93. - To show first position when trying to secure the last few degrees of supination.
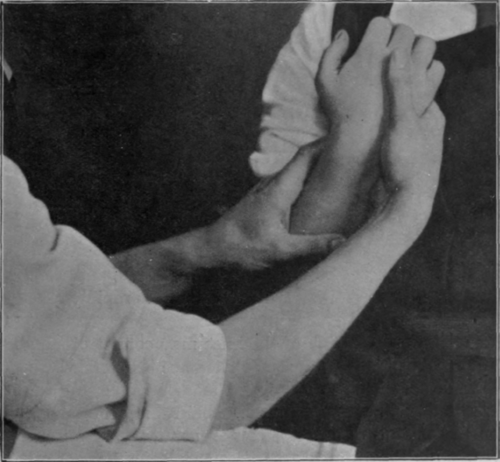
Fig. 94 - To show the second position when trying to secure the last few degrees of supination.
As examples of the beneficial effect of the repetition of forced movement may be cited the restoration of the last few degrees of supination of the forearm or extension of the knee. It is not uncommon to find that supination is complete when the elbow is fully flexed and somewhat deficient when it is extended. Supination is started with the forearm lying across the chest as if in a sling, it is increased as the elbow is flexed, and then it is maintained in this position while the elbow is rapidly extended (see Figs. 93, 94, and 95).

Fig. 95. - To show the final position when trying to secure the last few degrees of supination. The passage from the position shown in Fig. 94 to that here depicted should be rapid.
Exercises for extension of the knee may consist of standing, sliding-seat, or ladder exercises. The knee is extended with all the rapidity of which patient and masseur alike are capable. These and similar manoeuvres should only be attempted when the amount of unrestored movement is very minute. If attempted in the earlier stages disaster in some form or other is almost certain to follow.
When a joint is practically rigid, or when movement is limited by what seems clinically to be a solid block from any cause, nothing but prolonged tension or pressure will effect a cure. This may be supplied by splintage or by the use of a sling, with a measure of success that is quite unattainable by massage or manipulation, for the simple reason that the force thus supplied is constantly acting throughout the twenty-four hours instead of being applied for, at the outside, a forty-eighth part of that time.
One point always to bear in mind is that a joint may appear to be stiff simply because the muscles controlling it are wasted. It is no uncommon thing to find abduction of the arm limited to the amount that can be effected by rotation of the scapula, owing to inability on the part of the deltoid to assist in the movement. Restore the strength of the deltoid, re-educate it to contract, and full movement of the shoulder may follow without difficulty.
Continue to:
My Books

