(i.) The Mechanical Effect of Massage on the Circulation
Description
This section is from the book "Massage Its Principles And Practice", by James B. Mennell. Also available from Amazon: Massage It's Principles and Practice.
(i.) The Mechanical Effect of Massage on the Circulation
There are only two ways in which massage can produce a mechanical effect on the circulation. It may assist the venous return, or it may so act on the walls of the arterioles as to maintain or restore the tone of the vaso-motor system.
We know the results of mechanical stimulation of the un-striped muscle within the abdomen, and, arguing from these results, it seems not unlikely that restoration of tone, through the mechanical effect of massage on the circulation, is really due to a reflex response to mechanical stimulation of the unstriped musculature of the arterial system.
Direct mechanical assistance to the arterial supply of a limb by massage has, so far as I know, never been advocated.1
If we desire to influence the vaso-motor mechanism, we can scarcely expect that purely mechanical agencies will effect our object, save in one or other of two distinct ways. By assisting the venous return we can lessen the vis a fronte in the arterioles, and the blood can then pass through them more rapidly. Thus, presuming the blood-pressure to remain unaltered, a larger supply of blood will be required for the part under treatment, and the vaso-motor mechanism must be called into play to fulfil this want.
1 Recently I have seen centrifugal stroking of the femoral artery advocated for senile gangrene of the toes. The suggestion seemed so unworthy of consideration, and the argument so fallacious, that apparently I did not trouble to retain the article.
It is also possible to cause a dilatation of the arterioles by paralysing their muscle fibres, much in the same way that we can note a paralytic dilatation as the result of an ordinary bruise. The only differences are that the paralytic distension caused by massage is (or should be) very transient, while that due to bruising is far less so; and that after bruising there is a certain amount of actual extravasation of blood. The pathology is the same, and the healthy glow seen on the surface of the skin after percussion is due to paralytic dilatation of the skin vessels (cf. p. 56). To the healthy person the effect of heavy percussion after violent exercise or a Turkish bath is undoubtedly pleasing, but its therapeutic value seems to be problematical. Any form of massage, with the exception of surface stroking, may be performed with rapidity and vigour if we wish to impart a general "refreshing" sensation. This treatment should only be administered to those parts which are nearly or quite normal and healthy - never over muscles that are paralysed or in neurasthenia - and only for a very few moments at a time over any given spot. Otherwise fatigue, either local or general, is inevitable.
If it is desired to cause a local hyperaemia, as is often the case, it would seem easier and safer to attain our end by some other means than by the use of massage, such for instance as the hot bath - be it air or water - or by some form of Bier's congestive treatment. Massage should be used to improve the circulation through the part treated. Contrast bathing where a limb is held alternately in very hot and cold water, is an excellent device for providing what Robert Jones has described as "gymnastics for the arterioles."
If we decide, therefore, that we will cease all attempts intentionally to secure mechanical effect on the vaso-motor system,- to a certain extent it is unavoidable in some of our manipulations, - it only remains to consider how our massage is to assist the venous return, leaving any vaso-motor effect to be achieved either by the result of our action on the venous return, or in response to reflex stimulation of nerve or muscle.
To assist the venous return there is no call for the expenditure of any great effort: the lightest touch is all that is required to empty the superficial veins of arm or leg. There is little reason for supposing that the pressure in the deeper veins exceeds 5 to 10 mm. of mercury, while in most of them it is lower still, the pressure in the veins at the root of the neck being negative. It follows, therefore, that downward stroking over the veins of the neck, in the absence of back-pressure, can do little or nothing to relieve intra-cranial pressure by mechanical means. Yet this claim is often made. The advantage gained by increasing the downward suction must be problematical. The relief so frequently afforded by this movement can only be due to reflex action, and in practice we find that surface massage is at least no less effective than deep stroking in securing relief of the feeling of congestion.
Bearing in mind the effect of muscular contraction on the venous flow, it stands to reason that any attempt materially to assist the flow by massage is doomed to failure if the lumen of the vein has already been reduced to a minimum by muscular contraction around it. Thus our first law of treatment, if we are attempting to assist the venous flow, should be to ensure absolute relaxation of all muscles, not only in the part under treatment, but also throughout the various areas of the body which lie between the veins under treatment and the large veins in the region of the heart. If we are dealing with the veins of the leg, it is essential to see that all the thigh muscles are relaxed as well as those in the leg itself. Moreover, if the intra-abdominal pressure is raised by contraction of the abdominal muscles, there is a certain amount of obstruction to the flow of blood from the femoral vein into the external iliac vein; and it is therefore impossible to attain the maximum benefit from our massage of the leg unless the abdominal muscles are relaxed as well as those of the thigh. The effect of gravity should also be kept in mind, and so we find that, if we wish to do everything in our power to assist the return of blood from the foot, it is not sufficient that the patient should be seated with abdominal muscles relaxed, but he should be recumbent with thighs supported in a slightly flexed position. In this position gravity no longer opposes the venous flow, there is no increase of intra-abdominal tension due to muscular action, and the thigh muscles are relaxed.

Fig. 1. - To show contour of the muscles, the lower limb being at rest and supported. Note that the long axis of the "oval" formed is transverse.

Fig. 2. - The same as in Fig. I, the limb being supported only at the heel. The long axis of the "oval" becomes vertical.
If we examine a limb in which the muscles are completely relaxed, we find that it closely resembles a rubber hot-water bottle filled with water rather more fully than is usually the case. Thus the shape of the leg if at rest and in the horizontal position on a bed is, roughly speaking, oval with the long diameter transverse. If the heel only is supported by an assistant and the muscles are kept at rest, the oval shape remains, but the long diameter becomes vertical. In either case, assuming the muscles to be normal, voluntary contraction renders the contour roughly circular (see Figs. 1 to 4). In other words, the muscles, when in a state of relaxation, respond within the skin to the same laws that would control the position of fluid in a bag; while if they are contracted they assume a consistency which is almost impervious to external pressure. We see then that, having secured perfect relaxation of the muscles, a very slight degree of pressure is all that is required to press the blood out of the part in contact with the hand into the next proximal portion. This truth is further borne out if we remember that it is possible almost entirely to deplete a limb of its venous blood by simple elevation.
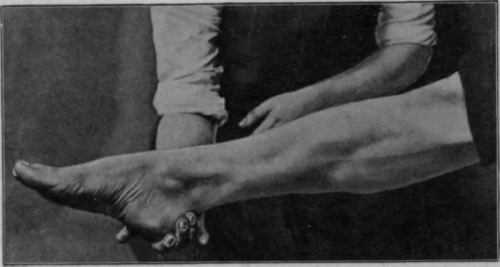
Fig. 3. - Contour with muscles contracted, the limb being supported only at the heel. The contour is more nearly circular than in Figs. 1 or 2.
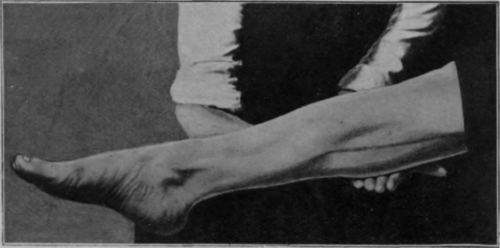
Fig. 4. - Contour with limb in same position as in Fig. 3, but with the calf supported. Note that the pressure on the calf now causes little or no change in the general outline of the limb, as the muscles are contracted.
If, on the other hand, we exert a considerable pressure in our movements, we shall empty the veins equally efficiently; but there are other blood-vessels to consider. The pressure in the arterioles is very low and in the smaller arteries not very much higher. By the application of any considerable amount of pressure in a centripetal direction, it is obvious that we shall be forcing the blood in these slender vessels against the direction of the flow; and it is difficult to argue from the purely scientific point of view that any benefit could result. Indeed, it is not inconceivable that we may be doing actual harm; we certainly cannot claim that by obstructing the flow of blood into the veins we are assisting the venous return, which is the main objective in our manipulations. The clinical effect of too heavy pressure is a blanching of the part under treatment. There is no reason to suppose that the vaso-constriction is confined to the skin-vessels; it must be presumed to take place in the deeper structures as well. Sometimes it is followed by a flushing of the part, due to subsequent vaso-dilatation, which if prolonged is probably paralytic (cf. p. 56). Anyone who has tested the blood-pressure in the brachial artery with an ordinary mercurial manometer will know how slight a grip of the bulb is required completely to obliterate the brachial pulse. It is true that in massage we do not apply our pressure to the whole circumference of the limb, and therefore we are not likely to attain a similar result by an equal pressure, but let us beware of doing so even in the smaller vessels.
Continue to:
My Books

