Anatomy. Part 3
Description
This section is from the book "Intra-Pelvic Technic OR Manipulative Surgery of the Pelvic Organs", by Percy H. Woodall, M. D., D.O.. Also available from Amazon: Intra-Pelvic Technic OR Manipulative Surgery of the Pelvic Organs.
Anatomy. Part 3
The pelvic colon begins at the superior strait of the pelvis and at about the middle of the third sacral vertebra becomes continuous with the rectum. Its average length is about sixteen inches, though it may vary from 4.8 inches to 33.6 inches and even in one case to 41.5 inches (Pennington). It is completely surrounded by peritoneum having a mesentery which is longer at its middle portion than at the ends, thus allowing this portion considerable range of motion. It is in relation anteriorly with the uterus and broad ligaments. Dr. M. E. Clark says it rests upon the fundus of the uterus. It often lies in the recto-uterine excavation, covered by coils of small intestines.
The rectum extends from the middle of the third sacral vertebra to a little beyond the tip of the coccyx. It is about five inches in length, and follows the curve of the sacrum. The lower portion of the rectum is dilated, forming the ampulla.
Anteriorly and laterally the rectum is covered by peritoneum for its upper two-thirds, but lower down only its anterior surface is so covered. The rectum is in relation anteriorly with the uterus, some coils of small intestines and frequently the pelvic colon unless a retro-displacement of the uterus be present. Lateral to the rectum are the ovaries, the fimbriated extremities of the uterine tubes and the ureters.
Coils of the small intestines can often be found in the recto-uterine excavation, unless this is already filled by the pelvic colon or a retro-displaced uterus. The small intestines are also in contact with the posterior or upper layer of the broad ligament and the upper surface of the uterus, unless as sometimes happens they are crowded out by the pelvic colon. (Fig. 4.)

Fig. 4. The Uterus and Its Relation to the Bladder, Rectum and Small Intestines.
The parovarium is the remains of the Wolffian body and the Wolffian duct. It is between the ovary and the uterine tube and is sometimes the source of origin of cysts.
Lying upon the pelvic fascia which covers the muscles forming the floor of the pelvis, is a variable amount of loose connective tissue. This serves as a sort of cushion for the viscera and a support for their blood vessels, nerves and lymphatics. This tissue is most abundant at the base of the broad ligaments, the sides of the upper portion of the vagina and about the cervix. It constitutes a large part of the ligaments of the uterus and in it ramify the uterine, ovarian, and tubal arteries and veins. In any condition causing pelvic congestion these vessels become enlarged. This connective tissue is frequently the seat of inflammatory effusions and exudates which may become organized and form cicatricial bands.
The peritoneum lining the pelvic cavity is a continuation of that, lining the abdominal cavity. Posteriorly it passes downward covering the pyriformis muscle and the sacral nerves, and embraces the upper third of the rectum. Passing on down it covers the anterior surface of the middle third of the rectum forming, as it passes from the rectum to the pelvic floor and from there to the upper portion of the vagina and on to the uterus, the recto-uterine excavation. It covers the uterus posteriorly and anteriorly as far down as the cervico-uterine angle. It passes on to the bladder forming the vesicouterine excavation, covering its anterior and posterior surfaces from which it is reflected to the anterior abdominal walls. The folds of peritoneum passing over the uterus posteriorly and anteriorly are reflected over the uterine tubes and form the posterior and anterior layers of the broad ligaments. Laterally the peritoneum forming the broad ligaments passes on to the sides of the pelvis.
Within the pelvic cavity peritoneal surfaces are continually in contact. When inflammation occurs, as it frequently does, the inflamed surfaces readily become adherent and form adhesions between the uterus and the surrounding viscera. Such adhesions are common sources of displacement or other pathological conditions.
The blood supply of the internal generative organs is so closely related that it is best considered collectively. It comes chiefly from the uterine and vaginal branches of the hypogastric and from the ovarian branch of the abdominal aorta. To a more limited extent the vesical, internal pudendal and middle hemorrhoidal branches of the hypogastric also supply these organs. A remarkable thing about these arteries, particularly the uterine and ovarian, is their tortuous course and the fact that these two form one large continuous anastomotic trunk. So intimate is their connection that during pregnancy.
It is claimed by some, the ovarian artery furnishes the principal blood supply to the uterus. They lie for the most part in the connective tissue between the layers of the broad ligament.
The venous system of the internal generative organs, in reality, forms one great pelvic plexus embedded in the connective tissue of the pelvis. Various parts of this plexus are named from their connection with some particular organ or from some other peculiarity.
The veins from the uterus arise from a network in its muscular substance from which they pass into a dense plexus at the sides of the organ. From this, the uterine plexus, are formed the two uterine veins which follow the uterine artery and return the blood to the internal iliac vein. The uterine plexus not only communicates above with the ovarian plexus and below with the vaginal and vesical plexuses but forms with them a continuous network of veins.
The veins from the ovary leave the organ largely from its hilum. These join with branches from the uterine plexus and from the uterine tube and form a dense valveless plexus, the pampiniform plexus, between the layers of the broad ligament. From this plexus the venous trunks arise which follow the arteries, the right ovarian vein opening into the inferior vena cava and the left ovarian vein into the renal vein at a right angle. These veins are imperfectly, if at all, supplied with valves, and the left one passing behind the sigmoid flexure of the colon is easily subjected to pressure when this viscus is filled.
The veins from the vagina form a plexus around this organ and freely communicate with the veins from the bladder, vulva, and rectum and become continuous with the great pelvic plexus. The veins from the uterine tubes enter the pampiniform plexus.
Especial attention is called to the pelvic plexus of veins because of its extent and location by the side of the upper portion of the vagina, along the margins of the uterus and the upper portions of the broad ligaments; its situation in the soft and yielding connective tissue of the pelvis; its practically valveless condition and its great dependence upon the aspirating power of the thorax for the onward flow of its blood. These conditions render these vessels very liable to engorgement as a result of any lesion affecting the vaso-motors of the pelvis or any condition affecting the general circulatory or respiratory systems.
The pelvic organs receive their nerve supply from the ovarian and hypogastric plexuses (sympathetic) and from the second, third and fourth sacral nerves (parasympathetic).
The ovarian plexus originates from the renal plexus. This in turn receives filaments from the coeliac, the aortic and the aortico-renal ganglia and is joined by the smallest splanchnic nerve. It follows the course of the ovarian artery and is distributed to the ovary and the fundus of the uterus.
The hypogastric plexus is formed by filaments from the aortic plexus and from the lumbar ganglia. It is placed between the two common iliac arteries in front of the fifth lumbar vertebra and the promontory of the sacrum. After sending some filaments to the fundus of the uterus it divides below into two portions situated at the sides of the rectum and vagina and called the pelvic plexuses.
The terminal branches of the hypogastric plexus with filaments from the (first and second) sacral ganglia, also from the anterior divisions of the second, third and fourth sacral nerves and from the nerves accompanying the uterine, ovarian and round ligament arteries, form the "pelvic brain" of Byron Robinson. This also called the "cervico-uterine" ganglion (Fig. 5), is a mass of gangliated gray matter situated on either side of the cervico-corporeal junction in the base of the broad ligament on a level with the middle of the cervix and about an inch lateral to it. Here it can easily be manipulated. Through it the nerves of the pelvic viscera are largely distributed. It is embedded in the pelvic connective tissue and through its gangliated cords, are intertwined arteries, veins and lymphatics. It is so intimately connected with the urinary, genital and lower intestinal tract that irritation in one is often reflected in the other two. The reader is referred to "The Abdominal Brain," by Byron Robinson.
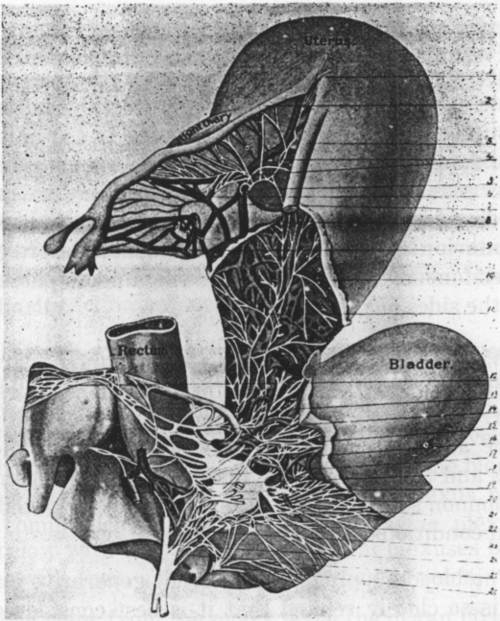
Fig. 5. The Nerves Of The Pelvic Organs Of Woman. (Frankenhauser.)
1. Nerves to fundus of uterus. 2. Right Fallopian tube. 3. Right round ligament. 4. Nerves to Fallopian tube. 5. Communication between uterine and ovarian nerves. 6. Ovarian plexus. 7. Ovarian vein. 8 Nerve, passing to ovarian plexus. 9. Fimbriated extremity of Fallopian tube. 10. Reflected peritonum. 11. Uterine nerves. 12. Superior hypogastric plexus. 13. Branches from hypogastric plexus to uterus. 24. Inferior hypogastric plexus. 15. Vesical nerves. 13. Communicating branches to vesical plexus. 17. Cervical ganglion. 18. Branches from hypogastric plexus to cervical ganglion. 19. First sacral nerve. 20. Branches passing to bladder. 21. Branches passing between bladder and rectum. 22. Communicating branches from second sacral to cervical ganglion. 23. Branch from third sacral nerve to cervical ganglion. 24. Second sacral nerve. 25. Branches from third sacral nerve to vagina and bladder. 26. Branches passing from fourth sacral to cervical ganglion (Garrigues).
Continue to:
My Books

