Downward Displacement. Part 2
Description
This section is from the book "Intra-Pelvic Technic OR Manipulative Surgery of the Pelvic Organs", by Percy H. Woodall, M. D., D.O.. Also available from Amazon: Intra-Pelvic Technic OR Manipulative Surgery of the Pelvic Organs.
Downward Displacement. Part 2
Pathology
The uterine ligaments are stretched and the vaginal walls are congested, thickened and inverted, in proportion to the descent. As a consequence of their congestion, thickening and increase in weight, they make additional traction upon the uterus and draw it further downward. In cases of complete prolapse the inversion may be so great that the vaginal walls are turned inside out, the uterus being inside the inverted vagina. Ulceration of the mucous membrane sometimes occurs. All of it that is exposed becomes dry, lustreless, thickened and resembles epidermis rather than mucous membrane.
The cervix, especially if it extends beyond the vulva, is eroded and ulcerated, if not from a primary laceration, then from friction against the clothing. The external os may appear normal or it may be gaping with its mucous membrane exposed.
Cystocele is a constant accompaniment, but rectocele is less so, as the anterior wall of the rectum follows the uterus down much less frequently than does the bladder. (Fig. 39.) The course of the urethra is distorted, passing backward and downward instead of upwards. Its orifice in complete prolapse may be found in the transverse folds on the upper part of the tumor.
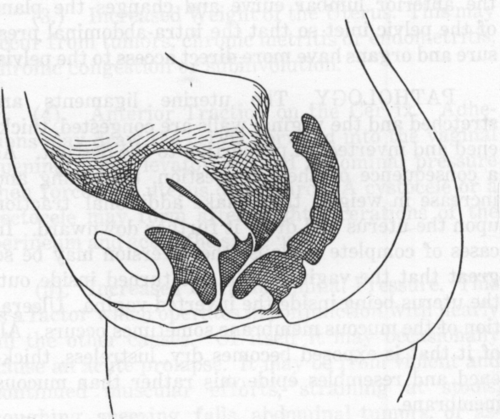
Fig. 39. Cystocele and Rectocele. Sectional View
In long standing cases the accumulation of urine in the bladder may lead to a chronic crystitis with hypertrophy of the vesical mucous membrane. This inflammation may extend to the ureters and even to the pelves of the kidneys. Prolapsus may cause an obstruction to the ureters, and acting in this way is the only uterine displacement which has been known to cause death.
The recto-uterine excavation usually extends down behind the prolapsed uterus to the lowest part of the tumor. It only occasionally contains some of the small intestines. The vesico-uterine excavation does not as a rule extend so far down.
Congestion of all the pelvic viscera results from the distortion of and obstruction to the blood vessels.
Symptoms
Marked cases of prolapse may exist without producing symptoms. In most cases there are pronounced bearing-down sensations, a feeling of weight and heaviness in the pelvis as if all the organs were going to drop out. These symptoms often occur when the prolapse is very slight, the socalled cases of "settling." There is difficulty in walking, discomfort on standing, pain in the back and loins, all which are increased by any muscular exertion sufficient to cause fatigue. The bladder empties incompletely or with difficulty, it sometimes being necessary for the patient to replace the cystocele through the vagina before it can be emptied at all. The retained urine decomposes and irritates the bladder and causes frequent and painful urination. Symptoms of a severe cystitis sometimes result.
The descent of the anterior rectal wall, or a rectocele, is not so common as the formation of a cystocele. When it does occur the feces may collect in the pouch thus formed and cause difficulty or pain on defecation, constipation and sometimes a slight proctitis.
Leucorrhoea is usually present but menstrual disorders are not marked, though menorrhagia sometimes results from the congestion incident to the displacement.
Conception may occasionally occur and take its normal course, the uterus prolapsing until its size retains it in position. Return of the prolapse usually occurs after confinement, but with care and attention during the period of involution a cure may be effected.
In cases of acute prolapse there is a sensation of something having given away, violent pain, shock, nausea, or vomiting, retention of urine, collapse, feeble pulse and clammy perspiration.
Diagnosis
In the cases of "settling" of the uterus a diagnosis may have to be made chiefly from the symptoms. Often very little derangement in position wall be found when the patient is examined in the dorsal posture. As a rule the uterus is found enlarged, boggy and unusually sensitive to pressure. If the patient is examined in the erect posture the descent of the organ can be determined. In the ordinary cases on vaginal examination the cervix will be found low down and pointing downward and sometimes forward as well. It may be within the vagina or protruding through the vulva. Bimanual examination will disclose the uterus as a whole lower than normal in the pelvis and retroverted as well. If completely prolapsed the uterus may be inspected and palpated as it protrudes from the vagina. It presents a smooth, dry surface with the vaginal rugae showing at the base of the tumor and the external os at its apex. On palpation a soft, elastic doughy mass of the characteristic shape of the uterus is felt within the inverted vaginal walls. In some cases of incomplete prolapse it is often necessary to examine the patient in the upright position, as in this position the maximum of prolapse will be evident. In the dorsal or Sim's position some degree of replacement may naturally occur.
A condition giving some of the physical signs of prolapse is caused by hypertrophy and elongation of the cervix. To differentiate them it is necessary to locate the body of the uterus by bimanual palpation. If the body is found high in the pelvis in its normal position the case is one of hypertrophy of the cervix. Cervical hypertrophy and prolapse may occur together, but in cervical hypertrophy the unusual length of the cervix will be discovered. The introduction of a sound disclosing the increased depth of the uterus will aid in this. It is impossible to replace the apparently displaced organ in a cervical hypertophy as can usually be done in prolapse.
A polypus or an inverted uterus may occasion some difficulty in diagnosis but in neither of these conditions is there an opening in the lower end of the tumor, while their small ends are upward, the reverse of a prolapsed uterus.
Continue to:
My Books

