1. Intussusception Or Invagination
Description
This section is from the book "A Manual Of Pathology", by Joseph Coats, Lewis K. Sutherland. Also available from Amazon: A Manual Of Pathology.
1. Intussusception Or Invagination
In this condition one portion of the intestine passes into another. In order that one piece may slip inside another, the one must present active peristaltic contractions, while the other is relaxed. The portion narrowed by the violent peristalsis passes inside of the relaxed part. This usually occurs in the natural direction of the peristalsis, but it may be reversed.

Fig. 394. - Twisting of the .sigmoid flexure. The upper limb has a much sharper turn than the lower, so that a flexible tube could be passed up from the rectum.
The condition is most frequent in children in whom the peristalsis is very active, and in whom also the large intestine is more freely movable than in adults.
These conditions are most frequently satisfied at the junction of the small and large intestines. The large intestine is naturally wide, and its peristaltic movements are sluggish. If then the ileum at its last part presents peculiarly violent peristaltic contractions it may pass into the large intestine as in Fig. 395. The invagination, however, is not usually a simple inversion of the ileum into the colon; in most cases the ileo-csecal valve is carried before the advancing ileum and forms the apex of the intruded piece. This implies that the caecum itself is carried inwards and inverted, and. the orifice of the vermiform. appendage is sometimes to be found near the apex of the invagination. The invagination is not infrequently very extreme, and the invaginated part may be carried right on to the rectum, so that the apex may be felt per anum.
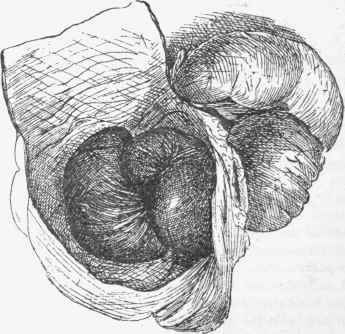
Fig. 395. - Intussusception. The colon is laid open and several coils of ileum are shown, which have protruded through the ileo-csecal valve. One of the coils was gangrenous.
Besides this form we also meet with invagination of the large intestine itself, one part into a succeeding part. It occurs but rarely in the small intestine. (See Fig. 396).
In the bodies of children, especially those who have died from cerebral or intestinal affections, we frequently meet with a form of invagination which has produced no symptoms during life, and has really occurred just at the time of death. It is usually present in the small intestine, where a small inversion of one part into a succeeding one is found. The invagination is easily reduced by slight dragging, and there are none of the secondary changes visible, such as are to be mentioned immediately as following invagination. Just at death, or immediately after it (as may be frequently seen in animals), the intestine commonly shows violent peristaltic movements, but these are irregular, and it readily happens that a much contracted part passes inside a relaxed portion.

Fig. 8SW. - Largo intussusception of small intestine.
When a piece of intestine is invaginated, there are three tubes, the outside one in its natural position, forming the sheath, the interna] one, which, although abnormal in position, runs in the usual direction, and the middle one joining the other two, and with its mucous surface directed outwards. There is frequently a more complicated condition than this, the intestine being tightly packed in several layers. The mesentery is carried in with the intestine, and by being dragged on at one side, it may give the gut a somewhat oblique direction. In the process of invagination the peritoneal surfaces are applied against each other as are also the mucous. It is characteristic of the peculiarities of these two structures that the peritoneal surfaces very readily coalesce and become permanently adherent, while the mucous surfaces do not.
The packing of intestine causes considerable interference with the circulation, and this is increased by the mesentery being partly included and its vessels pressed on. The obstruction to the calibre of the intestine is thus associated with hyperemia, cedema, haemorrhage, inflammation, and even gangrene, just as in an incarcerated hernia. The inflammation may lead to general peritonitis; or the separation of a gangrenous part may allow of the escape of the intestinal contents and lead to a fatal peritonitis. On the other hand, permanent adhesion may occur, between the sheath and the upper end of the included part, at the proximal extremity of the invagination, and, the inner and middle tubes becoming gangrenous, they may come away in whole or in part, as a slough, and the continuity of the intestine be restored with the loss of a piece. It is not usual for complete gangrene of the included tubes to occur, but what remains becomes adherent to the sheath, and, by contraction, gradually accommodates itself, and so the calibre is fully restored.
Continue to:
My Books

