2. Symptomatic Inflammations
Description
This section is from the book "A Manual Of Pathology", by Joseph Coats, Lewis K. Sutherland. Also available from Amazon: A Manual Of Pathology.
2. Symptomatic Inflammations
This class embraces the inflammations occurring in the acute fevers. In some the cutaneous affection is very trivial. Thus the eruptions in measles, scarlatina, typhoid and typhus fevers, consist of little more than inflammatory hyperaemia with slight exudation, but also, in severe cases of typhus, haemorrhages, forming petechias. The action of the irritant on the epidermis is evidenced in many cases by the subsequent occurrence of desquamation, which implies that the cells have been so injured as to lead to their premature necrosis and discharge. This occurs especially in scarlet fever and measles.
In Small -pox there is a much more severe inflammation. In this case the virus, consisting of micrococci which are present in the exudation or so-called lymph, evidently lodges in the skin and multiplies there, leading to pronounced local changes.
The effects of the irritant are seen mainly in the epidermis, which shows changes chiefly in the more plastic Malpighian layer. Many of the cells undergo a kind of coagulation-necrosis, their nuclei being lost and their substance converted into a hyaline material. These necrosed epidermic cells allow of spaces being formed among their layers in which exuded fluid collects. In this way a vesicle is formed, but it does not consist of a single cavity. As shown in Fig. 477, the epidermic cells or their remains form a network of fibres and partitions which divide the vesicle into compartments or loculi (b in figure) ii; which a serous fluid, containing the micrococci, is present. As the inflammation increases in intensity leucocytes are exuded, and these accumulate, as seen in the figure, both in the superficial layers of the cutis (d) and in the loculi of the vesicle. By the aggregation of these the vesicle becomes a pustule. In the figure it is seen that while the papillary layer of the skin (d) is somewhat infiltrated with leucocytes, yet it is not destroyed, and the interpapillary processes of the Malpighian layer of the epidermis (c) still persist. Sometimes no farther destruction occurs than this; the pustule dries in and a cruet is formed, and under it the Malpighian layer forms new epidermis, so that when the crust is shed healing occurs without any loss of substance. Hut more commonly the action of the virus causes death of the superficial layers of the cutis as well as of the epidermis. This is shown in Fig. 478, where an injection thrown into the arteries runs into the surrounding skin (a, a), but does not penetrate into the slough (b). In this case, when the crusts are torn, little sloughs infiltrated with pus are revealed, on the removal of which ulcers appear. By the healing of the flat ulcers we have the depressed reticulated cicatrices characteristic of small-pox (the so-called pitting of small-pox).
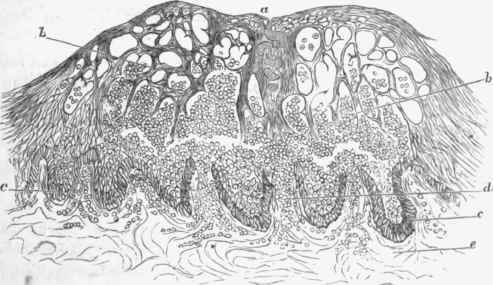
Fig. 477. - Section of a small-pox vesicle. Superficially there is a network formed of the altered epidermis. In some of the meshes (b, b) are pus corpuscles. For the most part the Malpighian layer in its deepest cells (c) is preserved, but at some points, as at d, it is broken through and the pus is infiltrating the skin, a, umbilication of the vesicle, due to a sweat gland, the coils of which are distinguishable, x 140. (After Rindfleisch).
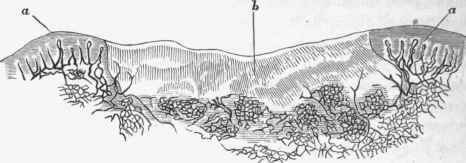
Fig. 478. - Small-pox eruption with necrosis, from an injected specimen. The normal skin at either side (a, a) has its vessels fully injected, while the necrosed part. (6) is uninjected and homogeneous, x 50. (Rindfleisch).
Vaccination produces a lesion identical in its anatomical characters with that of small-pox.
Continue to:
My Books

