4. Defective Closure Of Abdomen (Fissura Abdominalis)
Description
This section is from the book "A Manual Of Pathology", by Joseph Coats, Lewis K. Sutherland. Also available from Amazon: A Manual Of Pathology.
4. Defective Closure Of Abdomen (Fissura Abdominalis)
It is to be remembered that in the early foetus the anterior wall has a great gap to give transit to the umbilical vesicle and the allantois, and that it is by the gradual contraction of these structures that closure is rendered possible. As noted above, defective closure of the abdomen is sometimes associated with defect of the thorax. In complete fissure of thorax and abdomen, as there is no umbilicus, there is usually no proper umbilical cord, and the vessels pass, directly from the placenta by the amnion to the cleft in the abdomen. The proper abdominal fissure, in its highest degree, extends from the ensiform cartilage to the pubes. In that case the viscera are extruded, the urinary bladder is cleft, and the genital organs are absent or defective. Sometimes the" defect is less, and the abdominal contents lie outside the abdomen in a large hernial sac (see Fig. 11). The umbilical cord is usually absent, and the placenta is directly in contact with the sac, the vessels traversing the latter to reach the abdomen. Two special forms merit more particular attention.
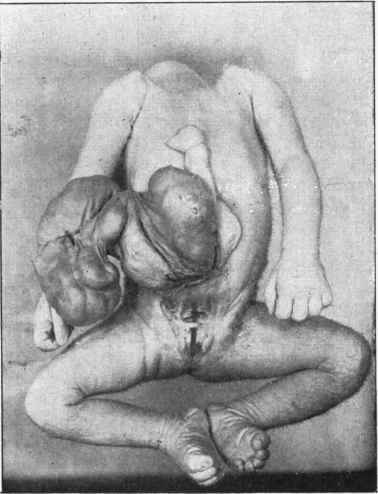
Fig. 11. - Fissura abdominalis. There is a sac containing protruded viscera, namely, intestine and part of liver. Below, the conditions are those of Assure of bladder. The long black rod is passed under a bridge which crosses the urethra. To the right of this rod below is a short rod, which passes into vagina; on either side are labia pudendi separated. Above, the small rods on each side are in the ureters.
(A) Hernia Of The Umbilical Cord (Hernia Funiculi Umblicalis)
This is really a minor degree of the condition last mentioned. There is, at the seat of the umbilicus, a rounded tumour, from the distal extremity of which the cord passes off, there being no proper umbilicus. The tumour consists of a peritoneal pouch which is protruded through the abdominal wall. There is an aperture in the wall of the abdomen, and the peritoneal pouch is covered with amnion, which is continuous on the one hand with the surface of the abdomen, and, on the other, with the surface of the umbilical cord. The hernia is one, therefore, of the umbilical cord, and not simply of the umbilicus. When the cord drops off, the amnion goes with it and the peritoneal sac-is exposed. If the tumour be large it will become gangrenous, and the patient will rapidly succumb. Even if the tumour be small the exposure generally results in fatal peritonitis, and it is only exceptionally that the gap in the abdomen is closed by healing.
(B) Fissure Of The Bladder (Inversio S. Extroversio Vesicce)
In this condition the abdominal wall between umbilicus and pubes is incomplete. The allantois has failed to close completely inside the abdomen so as to form the urinary bladder, and the lateral borders of the latter are adherent to the sides of the cleft, while the anterior wall is entirely absent. The posterior wall of the bladder therefore fills the cleft, and as it is pushed forward by the abdominal viscera it protrudes as a soft red area of mucous membrane, which readily bleeds, and on the surface of which the ureters open. At the upper end of the cleft is the umbilicus, which is frequently displaced downwards. The conditions shown in Fig. 11 are those of extroversio vesicae such as occur without the more complete fission shown in that illustration.
The defect generally extends to the parts below. The pubic bones do not meet in the middle line, the rami ending in rounded lateral prominences. In the female the urethra is usually absent as well as the clitoris, and sometimes the vagina is defective or absent. In the male there is a rudimentary penis, which is not traversed by a urethra, but presents on its upper surface a deep groove which represents the cleft urethra.
(C) Minor Degrees Of Incomplete Closure In Front
The cleft may confine itself to the upper part of the bladder, which presents itself as a red protrusion just beneath the umbilicus, the parts below being perfect. A still less degree is a simple persistence of the urachus. which then forms an open communication between the bladder and the surface at the umbilicus. We may also have a Cyst of the urachus from expansion of a partially obliterated urachus.
On the other hand it may be the lower part which is defective, the urinary bladder being well formed, hut the urethra cleft and otherwise imperfect. In the male this constitutes Epispadias. The penis is short and cleft on its dorsum, the urethra forming here a deep groove. The groove ends posteriorly in an aperture which communicates with the bladder beneath the pubes.
The causation of these malformations is obscure. It may be that there is a simple failure in the formative material of these parts, or that an over-distension of the allantois has prevented a proper closure.
Continue to:
My Books

