7. Malformations Of The Semilunar Valves
Description
This section is from the book "A Manual Of Pathology", by Joseph Coats, Lewis K. Sutherland. Also available from Amazon: A Manual Of Pathology.
7. Malformations Of The Semilunar Valves
Malformations of the aortic or pulmonary valves may be part of congenital lesions of the main vessels themselves, but are frequently of independent origin. The valve may be in the form of a diaphragm in which there are merely indications of a tripartite formation (see Fig. 201). In this case the diaphragm is often protruded into the vessel in the form of a funnel. Again, we not infrequently meet with some variety in the size or number of the semilunar folds. There may be only two curtains, usually a large and a normal one, the larger one commonly showing indications of a partial division (see Fig. 202). Then with three curtains there may be two large segments and a small rudimentary one between.

Fig. 201. - Congenital adhesion of the curtains of the pulmonary valve. The valve is viewed from above. (Peacock).

Fig. 202. - Congenital malformation of aortic valve. There are two curtains, but the larger one shows a partial division. (Peacock).
Many of these malformations are probably to be referred to endocarditis occurring in the foetus. In adult life endocarditis often produces adhesion of the curtains, but there is also very great contortion of the valves. But, in the foetus, the plastic power and adaptability of the structures is much greater, and the three coalesced valves may form a well-shaped diaphragm, or the two a single larger semilunar fold. In either case there are still indications of the coalescence in the form of thickenings along the line of union.
It is obvious that these malformations will frequently interfere with the functions of the valves. In the extreme cases of complete union of the three curtains (as in Fig. 201) there will be great obstruction as well as imperfect closure. When there are only two curtains, the middle part, where coalescence has occurred, is thicker, and the curtain may be more rigid at this point, and so its function will be interfered with.
According to Peacock, congenital malformations of the valves are apt to lead to more definite disease from endocarditis in after-life. This may be a recurrence of a foetal endocarditis, but, in addition, the imperfect adaptation of the valves will itself give rise to a certain irritation and predispose the structures to inflammation. So it happens that valves malformed in this way are peculiarly prone to disease in after-life, even though their function is not at first imperfect.
Besides the variations already noted the curtains of the aortic and pulmonary valves are sometimes abnormally numerous, especially those of the latter. There may be four curtains instead of three, and they may present all varieties of size relative to one another.
The semilunar valves sometimes present a condition somewhat approaching that of the cuspid form. It is to be noted that during the closure of a semilunar valve the curtains do not come in contact by their free margins, but that the line of contact is somewhat removed from the margin. During closure, therefore, when the artery is full, a certain portion of the curtain floats free in the blood. This portion between the line of contact and the free margin is frequently the seat of apertures or fenestrations, and that without affecting the function of the valve. This fenestration may be very extreme and may graduate towards a condition in which (see Fig. 203), instead of a piece of tissue, there is merely a series of tendinous bands passing from the curtain, near the line of contact, to the wall of the vessel at the point of insertion of the curtain. These tendinous bands resemble the chordae tendineae of the cuspid valves, and the resemblance may be increased by the neighbouring edges of the curtains being joined, and the tendinous bands from the adjacent borders of two curtains passing together to the wall of the vessel. There may be even on the wall of the vessel an elongated prominence into which the bands are inserted, and resembling a musculus papillaris (see figure). These bands may have a considerable free course from the middle of the curtain to the wall of the vessel. A certain amount of this condition is very frequent in both the aortic and pulmonary valves.
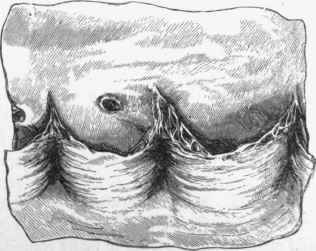
Fig. 203. - Fenestration of the marginal parts of the aortic valve. There is an appearance of chordae tendineae, and the bands from two proximal curtains are inserted into a projection from the aorta.
It may be asked, Does such a malformation interfere with the function of the valve? Probably not much, but still to a certain extent. Each form of valve is appropriate to its own place. The cuspid form is adapted to an aperture between two cavities, the semilunar to the orifice or course of a vessel. The latter takes up less room, as in it, by reason of their complete separation, the curtains fall back completely when the blood rushes past. But if the valve approaches to the cuspid form, especially if the margins of the curtains are united, and the tendinous bands from two have a common insertion, then there can hardly be that complete falling back which occurs when the structure is perfect. This will probably cause a trivial obstruction, but the curtains being unduly exposed to the force of the wave of blood may be specially liable to inflammation.
Continue to:
My Books

