Forms Of Bright's Disease. Part 3. (B) Interstitial Nephritis (Granular Contracted Kidney, Cirrhosis Of The Kidney)
Description
This section is from the book "A Manual Of Pathology", by Joseph Coats, Lewis K. Sutherland. Also available from Amazon: A Manual Of Pathology.
Forms Of Bright's Disease. Part 3. (B) Interstitial Nephritis (Granular Contracted Kidney, Cirrhosis Of The Kidney)
This form of nephritis is for the most part chronic throughout, although sometimes an acute nephritis may pass into it, and it may even ensue on a scarlatinal nephritis. It is chiefly characterized by changes in the interstitial connective tissue, but there are also lesions in the glomeruli, blood-vessels, and tubules. Weigert suggests that the primary changes here may be in the secreting structures, the affection of the interstitial tissue being secondary.
The interstitial tissue shows, throughout the cortex, a general increase, and it is unduly cellular; but there are also special areas in which the cells are in great excess. These areas are uniformly distributed throughout the kidneys, are usually wedge-shaped with the base at the periphery, and correspond with the regions of convoluted tubules. Whilst there are thus multiple areas in which the inflammation, apparently local from circumstances of structure, is more concentrated, the general connective tissue is increased and shows a coarse fibrous character, markedly different from the normal. The new-formed tissue in the cortex is continuous with the capsule of the kidney and renders it adherent, so that sometimes it is impossible to remove the capsule without tearing the kidney tissue. The connective tissue possesses the contracting character usual in such tissue, and this has an important effect especially on the tubules and capillaries.
The uriniferous tubules in the areas in which contraction has occurred are dwarfed (Fig. 428). In less affected parts, on the other hand, they are frequently dilated, there being here a kind of complementary dilatation. There is thus frequently visible a group of dilated and convoluted tubules (Fig. 429, b). The loops of Henle are also dilated, and by the shrinking of the cortex may be doubled up and rendered tortuous (Fig. 429, c). The epithelium in the dilated tubules is frequently fatty. Tube casts are also present in the tubules, and they may be very abundant. They are usually hyaline in appearance, and are occasionally present in the tubules both of cortex and pyramids.
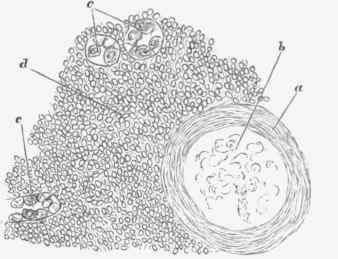
Fig. 428. - Interstitial nephritis. .Sclerosis of glomerulus, a, thickened capsule; b, condensed vessels of tuft; d, abundant round cells in interstitial tissue; c, dwarfed tubules remaining, x 350.
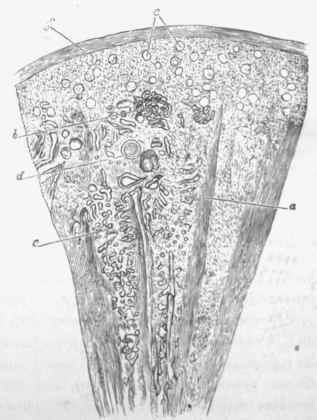
Fig. 429. - Section of contracted kidney with a Terr low magnifying power. (This should be compared with Fig. 417, p. Ml, similarly magnified.) a, medullary rays; b, convoluted tubules crushed together and dilated; c, region of artoriic rectoe and loops of Henle, the latter dilated and forming cysts; d, largo artery between pyramid and cortex, showing endarteritis obliterans the space between this and surface represents the cortex. and may be compared with similar spacs in Fig. 417: e, glomeruli, closely set and contracted, they also present a white homogeneous appearance; f, capsule.
Cysts are of very frequent occurrence in the contracted kidney. They arise mainly from the tubules by still further dilatation, and they very commonly lie together, sometimes in rows, as if from the crushing together and obstruction of a single tubule. Cysts also arise sometimes from the glomeruli, by the accumulation of fluid inside the capsule. All these cysts arise by obstruction of the tubules, and the usual contents are a watery fluid, but sometimes colloid matter is contained in them, apparently arising by secretion from or transformation of the epithelium. In nearly all cases there are cysts visible to the naked eye, and they are frequently so visible in large numbers. But many of them are microscopic in size.
By these processes great dislocation of the kidney tissue results, so that instead of the perfectly regular arrangement of the normal kidney, such as is shown in Fig. 417, p. 931, there is at once great shrinking and great distortion, as shown in Fig. 429 (drawn by the same apparatus and similarly magnified).
The capillaries are greatly pressed on by the shrinking connective tissue and greatly obliterated. There is, in many cases- in this way, a very great reduction in the capillaries of the kidney.
The glomeruli are also strikingly altered. The first change is a thickening of the capsule (Fig. 428, a), which shows concentric fibrous layers. The tuft of vessels is subsequently occluded and converted into a dense homogeneous nodule. In this way the glomerulus is greatly contracted, being often reduced to less than half its normal size, and is represented by a solid white glancing nodule in which can still be recognized, as a rule, the thickened capsule presenting its concentric fibrous appearance (a in figure), and the central more homogeneous-remains of the vessels (b in figure). This condition is commonly called Sclerosis of the glomeruli, and the resulting appearance is very striking, especially as, with the atrophy of the tubules and contraction of the fibrous tissue, the altered glomeruli are commonly brought close together.
The Blood-vessels take part in the inflammation, especially the Arteries. Their external coat, being continuous with the interstitial tissue, is thickened along with it. In addition to that, however, the internal coat is usually very markedly thickened. This thickening of the internal coat, which has the characters of Endarteritis obliterans (see Fig. 247, p 487), affects chiefly the ascending and afferent arteries of the cortex, but may also be present in the larger arteries between cortex and pyramids. It is sometimes so great as almost to amount to obliteration, of the arteries.
It may be a question to what extent some of the other lesions are due to this narrowing of the arteries. We shall see further on that a primary obstruction of the arteries may lead to atrophy of the tissue and sclerosis of the glomeruli, and, according to Leyden, the lesions in the kidneys produced by lead-poisoning are due to a primary narrowing of the arteries. It may be said, however, in general, that when atrophy is due to a primary endarteritis the affection is localized according to the accidental distribution of the arterial affection, whereas in interstitial nephritis the affection altogether is diffused and homogeneous, which is the regular fact in ordinary chronic Blight's disease.
Naked-Eye Appearances
The granular contracted kidney is usually small, dense, and tough, and the two kidneys not infrequently show a considerable difference in size. There may be in the early stages some enlargement, and a condition designated large red kidney has been described. The reduction in size varies greatly; in the most extreme degree the kidney weighs about two ounces. The kidney feels dense, and on section it is found to be tough. The capsule is firmly adherent, so that on removing it small portions of tissue come off with it. The surface has a general red colour, and is almost homogeneously granular. The prominent parts represent the less shrunken portions, and there may be some opaque markings from fat in them.
On the cut surface the regular normal appearance is greatly altered. The cortex is greatly thinned, sometimes forming only a thin rind, scarcely more than a twelfth of an inch in thickness between the bases of the pyramids and the surface. The cortex has lost all its normal markings, and it is indefinitely demarcated from the bases of the pyramids. These changes may be partly appreciated by comparing Figs. 417 and 429, where d represents in both figures the vessels at the bases of the pyramids, and the cortex is the part between them and the surface. Cysts are also visible on examining the surface.
Continue to:
My Books

