VII. Necrosis Of Bone
Description
This section is from the book "A Manual Of Pathology", by Joseph Coats, Lewis K. Sutherland. Also available from Amazon: A Manual Of Pathology.
VII. Necrosis Of Bone
Death of bone is of frequent occurrence, and it leads to such obvious phenomena that the term necrosis has been almost monopolized by mrgeons for this condition.
Causation
Necrosis in bone is nearly always the result of interruption of the blood-supply. From its frequency it might be supposed that bone readily succumbed to such deprivation, but the reverse of this seems to be the case. Macewen's observations in regard to transplantation seem to show this. (See under Transplantation.) Bone receives its supply of blood partly through small vessels which. pass from the periosteum and partly by larger vessels, of which there is generally a special one for each bone, which penetrate the bone and are distributed from within, such vessels being specially named the nutrient vessels.
Necrosis is mostly brought about by the periosteum being raised, sometimes traumatically, but generally as a consequence of inflammation, especially when pus accumulates between the membrane and the bone. As inflammation coincides the irritant producing the inflammation will in many cases have its share in causing the necrosis. By the raising of the periosteum the periosteal blood-supply is cut off, and the nutrient vessels may also be severed. According to Macewen the supply of the nutrient vessel of a long bone is generally sufficient to keep the bone alive even when the whole periosteum is stripped. This author records a case in which the whole diaphysis of the tibia was denuded of periosteum, but in which the persistence of the nutrient vessels caused all the bone to survive except a small superficial scale.
Necrosis is an occasional result of inflammation in the bone itself, and it occurs in the form of caseous necrosis in tuberculosis. Injuries, by separating a portion of bone, will sometimes produce necrosis, and will do so almost inevitably if septic processes coincide.
Resulting Conditions
The dead piece of bone is in itself inert, and undergoes merely passive changes. It retains its form and general appearance, but if it remain long, being macerated by the juices of the body, it assumes the characters of macerated bone. It then appears white and dry, and, as it contains little organic matter, it feels hard to the probe and gives a sound on being struck.
Inflammation is a constant concomitant of necrosis. If the latter has not been due to inflammation, then it leads to it secondarily. The dead piece of bone seems to stimulate the surrounding living tissue, and to lead to a chronic inflammation. By means of a rarefying ostitis the Haversian canals and medullary spaces enlarge and the bone immediately around the dead piece being replaced by granulation tissue, the necrosed piece becomes a Sequestrum.
At the same time new-formation commonly occurs, chiefly in the subperiosteal tissue, which has probably been separated from the dead bone, but also in the medulla. There is thus produced an irregular layer of new bone, as shown in Fig. 272. This new bone is largely subperiosteal, and in many cases it forms an external shell which may exercise the function of support instead of the bone which has died. This external shell frequently confines the dead piece, rendering it difficult of access for removal by the surgeon. It is generally provided with apertures called Cloacae through which the pus of the original suppuration has passed, and which have remained as canals or gaps in the new-formed shell.
The ultimate disposal of the dead bone occurs in different ways according to circumstances.
Absorption of dead bone is of frequent occurrence. In simple fractures it is probable that detached pieces of bone frequently die and become absorbed. Similarly in compound fractures pieces are not infrequently visible in the wound, having the dead white colour and hard feeling of sequestra, but if the wound remains aseptic they are absorbed. Again, at the ends of stumps sequestra often form, and they are sometimes, at least partially, absorbed. In all these cases, and even in acute infective ostitis, the dead bone may be absorbed if septic changes be averted or overcome.
The absorption is effected by the Osteoclasts. In Figs. 273 and 274 the appearances are shown as observed by the author in a case of limited necrosis at the end of a stump, in which absorption was in progress. Here the Haversian canals and medullary spaces as seen in Fig. 273 are enlarged, and their borders have a worm-eaten appearance. This latter is shown in Fig. 274 to be due to the existence of Howship's lacunae, in which are giant cells exercising their function of osteoclasts. Sometimes a regular row of such cells was visible, as if feeding on the bone, and they were occasionally almost buried in flask-shaped spaces (as at the left in Fig. 274). By this process bone may be entirely absorbed.
A similar process of absorption occurs, not only in pieces of bone which have died in the body, but in pieces of ivory or bone which have been introduced for therapeutic purposes, such as ivory pegs used in cases of ununited fracture, bone drainage tubes, etc.

Fig. 272. - Necrosis of femur. The smooth necrosed piece is seen with irregular new-formed bone around.
Absorption does not occur where the dead bone, having become septic, is itself a source of serious irritation. Thus a piece of dead bone may lie for years in a suppurating cavity almost unchanged. Cornil and Ranvier, for example, figure a transverse section of a sequestrum of the femur which had remained thirty years bathed in pus. In this time it had undergone no corrosion and had all the characters of macerated bone. The position of the sequestrum inside the shell of new bone often causes its retention, and its removal is only effected In-partial destruction of the external shell.

Fig. 273. - Section of a piece of necrosed bone which had been undergoing absorption. The margins of the bone at the medullary spaces and Haversian canals'have an eaten-out appearance from the presence of Howship's lacunae, x 80.
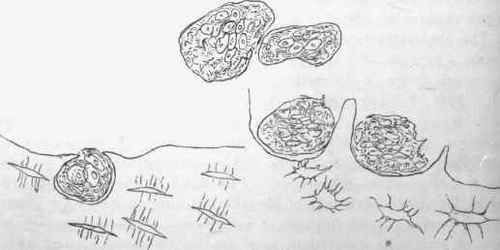
Fig. 274. - Howship's lacunae with giant-cells (osteoclasts) in them, and free giant-cells. From same piece of necrosed bone as preceding figure, x 350.
Phosphorus-Necrosis
This condition occurs chiefly in persons who are employed in workshops where lucifer matches are manufactured, and who are thus exposed to the vapour of phosphorus. The vapour acts locally, on the jaws chiefly, and it is said that persons with carious teeth are particularly liable to be affected. The phosphorus produces an inflammation mainly of the periosteum, resulting in a great new-formation of cancellated bone on the surface of the jaw. This bone may afterwards become condensed by the ossification encroaching on the medullary spaces. After a time the inflammation leads to suppuration, the pus forming between the new-formed bone and the original bone of the jaw. From this results a necrosis of the jaw which may involve the entire bone, and may extend to the new-formed bone. The resulting suppurations are usually fatal, but after removal of the sequestrum healing may occur. Microbes of various kinds are present in the pus. In the discharge from six cases recently examined by Stockman the tubercle bacillus was found.
From the observations of Wegner it appears that phosphorus acts as a general stimulant to the structures concerned in the formation of bone. The phosphorus vapour acting directly stimulates so violently as to produce the inflammation and necrosis just described, and this result has been produced also in rabbits exposed to the vapour of phosphorus. When given in small doses internally, phosphorus produces in growing animals a distinct stimulation of the process of formation of bone. In such cases the bone produced at the ossifying border of the cartilage is not a spongy bone, but a dense layer, and there is also an unusually dense bone produced beneath the periosteum. It is noteworthy that in growing animals to whom small doses of phosphorus were given, while insufficient quantities of lime were supplied, there was a great production of osteoid tissue, somewhat like that • produced in rickets.
Literature
Macewen, Annals of Surgery, 1887; Wegner, Virchow's Arch., lvi., 1872; Coats, Glasg. Med. Jour., vi., 1874; Bibra und Geist, Krankh. d. Arbeiter in der Phosphorfabriken, 1847; Trelat, De la necrose causee par le phosphore, 1857 Thiersch, Arch. d. Heilk., 1868; Wegner, Virch. Arch., lv., 1872; Cameron. Glasg. Med. Jour., xvi., 112, 1881; Haeckel, Langenbeck's Arch., xxxix., 1890; JOST, Brun's Beitriige, xii., 1894; Stockman, Brit. Med. Jour., i., 1899.
Continue to:
My Books

