Arteries, Vein's And Nerves Of The Rectum And Anus

Description
This section is from the book "Diseases Of The Rectum And Pelvic Colon", by Martin L. Bodkin. Also available from Amazon: Diseases of the rectum and pelvic colon.
Arteries, Vein's And Nerves Of The Rectum And Anus
The Superior Hemorrhoid Artery, derived from the inferior presenter, divides into two branches descending along the posterior wall of the rectum. This artery, at about the level of the promontory of the sacrum, gives off the lower sigmoid which supplies the lower portion of the sigmoid flexible. The superior hemorrhoid gives off a number of branches which Anastasia with each other and with the middle hemorrhoid, and quite often with the inferior hemorrhoid arteries. The main branches of this artery take a parallel course.
The Middle Hemorrhoid Artery supplies the middle third of the rectum and has its origin from either the hypo gastric, pro static or the anterior division of the internal ilia arteries. It descends to just above the elevator an muscle, which it supplies within the pelvis-rectal space. This artery supplies sufficient blood to the lower end of the rectum to maintain its vitality, when the superior hemorrhoid artery is injured.
The Inferior Hemorrhoid Artery. This artery takes its origin from the internal pubic and traverses the mischief-rectal Fosse from the posterior outer wall, supplying the lower portion of the elevator an, the sphincter muscles, the skin and the superficial fascia of the anal margin. The branches of one side communicate with those of the other, and Anastasia with branches of the middle hemorrhoid artery.
The Middle Sacral Artery arises from the aorta posterior at its bifurcation. It descends along the middle line just in front of the sacrum and terminates in the gland of Luscious. It supplies the posterior surface of the rectum and anatomizes with branches of the superior hemorrhoid and lateral sacral arteries.
The Veins. The corresponding names are applied to the veins which return the blood through the portal vein and the inferior vane cave. The superior or internal hemorrhoid veins terminate through the presenter in the portal vein.
The middle and external hemorrhoid and the middle sacral veins convey the blood from the outer portion of the rectum and anus, discharging it into the vane cave. The internal hemorrhoid veins form a plexus which supplies the rectum proper, limited by the anew-rectal line. Below this line the external veins are located.
The veins of this region are not supplied with valves and therefore congestion from local or hepatic diseases often results in hemorrhoids. The superior hemorrhoid veins pass upward from Hintonâs while line to a distance of about three inches, just beneath the mucous membrane, then perforate the muscular coat and pass to the outside of the bowel.
Verne claims that these muscular button-holes contract around the veins and prevent the return of blood to the liver, causing hemorrhoids. The internal hemorrhoid plexus begins practically at the anew-rectal line, in the form of little pools, arranged like clusters of grapes, surrounding the columns of Morgan.
The Nerves of the Rectum and Anus originate from the sympathetic and cerebrums - spinal systems. Branches of the Presenter, hypo gastric and sacral plexus of the sympathetic,largely supply the rectum proper. The mucous membrane of the rectum becomes progressively more sensitive from above, downward, possessing very little sensation in the upper portion.

Fig. 3. Showing external and middle hemorrhoid veins from lower end of the rectum and anal canal. Branches also run upward to form the superior hemorrhoid veins.
The longitudinal and circular muscles of the rectum are supplied from the second, third, fourth and fifth sacral nerves. The elevator an is supplied by the third and fourth sacral nerves. The external sphincter muscle receives its nerve supply from the third, fourth and fifth sacral nerves which extend across the mischief- rectal Fosse. The spinal nerves convey motor impulses to the longitudinal muscular coats but inhibitory impulses to the circular fibers.
The Lymphatics of the rectum and anus are formed from two systems - an external, which drains the skin and anus and empties into the inguinal, and the internal or distinct rectal system, which empties into the sacral-lumbar glands. This division explains the origin of infection of the inguinal glands from a superficial abscess around the anal region and the involvement of the deep lymphatics in cases of malignant disease of the rectum proper. They seem to be arranged similarly to those in the large intestine generally, that is, in a system comprising three plexuses - one for the mucous coat, another for the muscular and one for the serous coat.
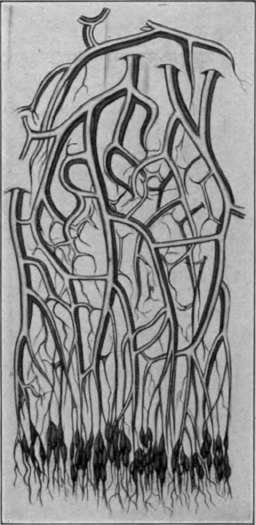
Fig. 4. Venous pools in which internal hemorrhoid plexus arises (schematic).
The muscular and serous plexuses drain into one another and into the adjacent glands, but the lymphatics from the mucous coat do not communicate with either of these before emptying into the adjacent glands. An important point to remember here is that the glands are found in two situations - in the hollow of the sacrum, and close to the gut. The lymphatics which lie along near the superior hemorrhoid vein and its branches pass first into the adjacent glands, while the efferent lymphatic stream from these glands passes to the glands which are situated on both sides, internal to the anterior sacral framing in the hollow of the sacrum. It is supposed that some of these lymphatics pass directly to the internal ilia glands.

Fig. 5. Lymphatics of superficial anal region.
The Sigmoid Flexible
The Sigmoid Flexible is generally described in recent anatomical text-books as consisting of two parts, an ilia and pelvic colon.
The Iliad Colon is described as that portion of the descending colon extending from the left ilia crest to the brim of the pelvis; the pelvic colon that part which extends from the brim of the pelvis to the promontory of the third sacral vertebra.
The ilia colon passes downward in the left ilia Fosse to a point just above Forepartâs ligament, it then turns inwards above the soaps muscle where it becomes the pelvic colon.
The ilia colon has no dysentery usually, and the peritoneum covers only its sides and anterior surfaces. Sometimes just at the commencement of the pelvic colon it may possess a dysentery. It lies upon the soaps and Iliads muscles, measures about five or six inches in length and is usually covered by some portion of the small intestine, excepting when it lies lower. When distended it may reach the abdominal wall.
The Pelvic Colon is continuous with the ilia colon, as stated above, and commences at the inner side of the left soaps muscle, forms a loop, then turns downward to become the rectum opposite the third sacral vertebra. It varies much in length, measuring as a rule sixteen inches, and possesses a dysentery which is usually about five inches in length, but may be found to measure from two to ten inches. The dysentery is attached to the pelvic wall, and can be traced backward to the sacral-ilia junction then downwards and inwards to the median line where it terminates at the third sacral vertebra. This loop of gut is freely movable and found often in different locations. Commonly it lies in the pelvis where at its beginning it crosses the external ilia vessels, and rests upon the uterus of the female or bladder of the male.
The bowel presents some different relations in the infant, as the greater part of the pelvic colon is situated above the pelvic brim. Owing to the sigmoid loop crossing from left to right the colon usually enters the pelvis on the right, instead of the left side. The rectum is proportionately larger and straighter in the child than in the adult. The peritoneum reaches as low as the prostate usually, in the male infant.
Continue to:

My Books

