Fissure In Anal. Continued

Description
This section is from the book "Diseases Of The Rectum And Pelvic Colon", by Martin L. Bodkin. Also available from Amazon: Diseases of the rectum and pelvic colon.
Fissure In Anal. Continued
Surgical treatment consists of dilatation, excision, and division.

Fig. 48. Fissure in anew Bilateral incision.
Dilatation, or stretching of the anal orifice by forcible or gradual means, has been in vogue for many years, especially among the French surgeons. Both of these methods have for their object the breaking up of the continuity of the muscle fibers or nerve strands, thereby relieving the muscular spasm. Dilatation is very painful under local anesthesia and one has only to try to dilate the anal canal of one of these sufferers to condemn the method, as the hypodermic injection is terrifying to them. Dilatation under general anesthesia is practiced commonly by surgeons and the results are most satisfactory. The anal dilators used generally are the hard rubber, wax, the Wales hollow graduated soft rubber bogies and the Kelly conical dilator. These dilators are used either with local anesthesia or often without any form of anesthesia.
However, forcible revulsion with the index fingers or thumbs is the most popular method of dilating, but should be accomplished only under a general anesthetic. Dilatation by any means is intended to over-stretch or rupture the sphincter muscles, thereby preventing their contraction, which is supposed to permit the healing of the ulcerated surface. To contradict this idea it is a well-known fact that the muscle regains its contractile power within a few hours or days, so that the relief is very temporary in most instances. Sometimes the extreme dilatation causes permanent incontinence. Healing will often follow dilating by any of these procedures, if a tube is left in the canal for from five to seven days afterward
This method of treatment is not certain, as a splitting of the muscular fibers may happen at any point in the circumference of the anal ring, which adds a traumatize to the previous pathological injury. Incision or excision are preferable on account of the definite area cut with the knife.
Excision consists of making an elliptical incision which circumscribes the fissure, permitting its entire removal. The wound may then be permitted to heal by granulation, or closed at once with catgut sutures. The latter method, however, is open to objection on account of the liability to infection under the sutures.
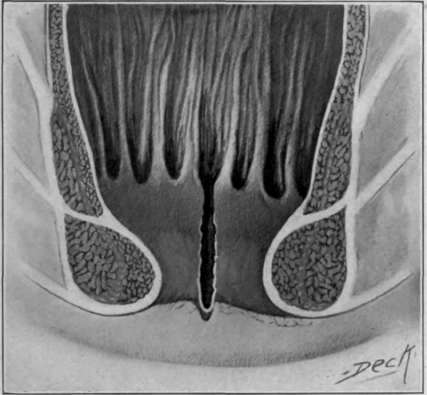
Fig. 49. Tear in crypt of Morgan producing fissure.
Incision. The extent of incision of the external sphincter for the relief of a fissure has been discussed for many years and seems not to have been settled yet. Each author advocates his or antherâs method, all of which vary as to the degree of incision, so that it appears to make little difference which method is used, if the surgeon limits his incision to the external sphincter only. The object and result must be the severance of the muscular fibers which act upon the diseased area. The incision can, therefore, be one which completely severs the muscle or that only penetrates it beyond these fibers, setting it at rest. The incision thus made should be through the ulcer, and can be applied to a fissure at any point in the circumference of the anal canal.
The incision for the posterior fissure which appeals to me and has proved most successful, is the bilateral, made on each side directly transverse to the sphincter fibers, and a little deeper and longer than the ulcer. This double incision puts at rest both sides of the muscle fibers over which the ulcer is situated.
Post-operative treatment of these cases consists in the application of tincture of iodine and stimulating with an ichthyology solution or balsam of Peru, applied either with the cotton applicator or on a piece of gauze inserted into the wound every day. Pure ichthyology or a five to ten per cent. solution of nitrate of silver may be necessary in severe cases.
Finally, if we consider that the fissure is secondary to a catarrh inflammation of the rectum, irrigation of the rectum is indicated every second day, as suggested for colitis. To bear out this theory, cases which were irrigated with a twenty per cent. solution of Kramer have healed nicely when combined with local treatment, without operation. These cases were not of the mild type and indicated incision for their relief from the surgical standpoint. There is no doubt in my mind that a healthy healing of the majority of fissures will follow correction of the digestive disturbances and the catarrh inflammations of the colon or rectum in this manner. A hypertrophy or strophic catarrh inflammation of the colon, sigmoid or rectum is in almost every instance the primary factor in its causation. The mucous discharge accompanying these diseases irritates the anal canal and interferes with the healthy granulation of an otherwise insignificant tear in the mucous membrane.
Continue to:

My Books

