Oesophagoscopy
Description
This section is from the book "Diseases Of The Stomach", by Max Einhorn. Also available from Amazon: Diseases of the Stomach.
Oesophagoscopy
Oesophagoscopy in the diseases of the oesophagus and cardia has gained an important place in the last few years. All the literature of importance on this subject will be found in an article1 published by me in the year 1897, regarding the inspection of the oesophagus and cardia. Further important papers on oeso-phagoscopy are those of Von Hacker,2 Rosenheim,3 and Gottstein.4 Von Hacker's epoch-making labors show most clearly the high and practical value of this method of examination, which not only facilitates the diagnosis of many of the diseases of the oesophagus, but frequently exerts a direct influence upon their treatment.
1 Laker: "Ueber ein rhytmisches Klaugphanomen des Mugcns." Wiener med. Presse, 1889, Nos. 43 and 44.
In the instruments used up to now for oesophago-scopy (Mikulicz, Rosenheim, Kelling) the source of the illumination is outside of the oesophageal tube. As a rule, the panelectroscope is employed for this purpose, an instrument that throws concentrated light through the whole tube, thus illuminating the lowest spot that is to be inspected. It is evident that inspection would be easier if the lamp were placed at the lower end of the tube near the area to be examined, since a better illumination could in this way be secured. With the appearance of the so-called "cold lamps" this principle could be practically executed.
The oesophagoscope which I use5 consists, as the accompanying drawing (Fig. 5) illustrates, of a round, hollow metal tube (A), having on one side a small longitudinal groove (2?), which is separated by a thin wall from the lumen of the tube. Two isolated electric wires attached to a carrier (F)1 run through the groove (B). At their end a small lamp (G) is attached and placed a little above the end opening of tube (A), being, however, not inclosed by the thin metal sheet that covers the wires. To the tube are attached a handle (C), a plug (D), and an obturator (E).
1 Mux Einhorn: "The Inspection of the (Esophagus and Cardia." New York Medical Journal. December 11, 1897.
2 Von Hacker: "Die Oesophagoseopic und ihre klinische Bedeutung." Beitrage zur klinischen Chirurgie, Bd. 20, 1898, p. 141; "Die Oesopha-goscopie beim Krebs der Spciserohrc und des Mageneingangs." Ibid., p. 275; "Ueber die Entfernung von Fremdkftrpern aus dcr Speiserohrc mittelst der Oesoplmgoscopie." lbid., Bd. 29. p. 128. 1901.
3Theo. Rosenheim: "Ueber Oesophagusstenose." Deutsche Klinik, 1901.
4Geo. Gottstein: "Oesophagoskopie," Jena, 1901.
5Max Einhorn: "A New Oesophagoscope." Medical Record, January 25th. 1902.
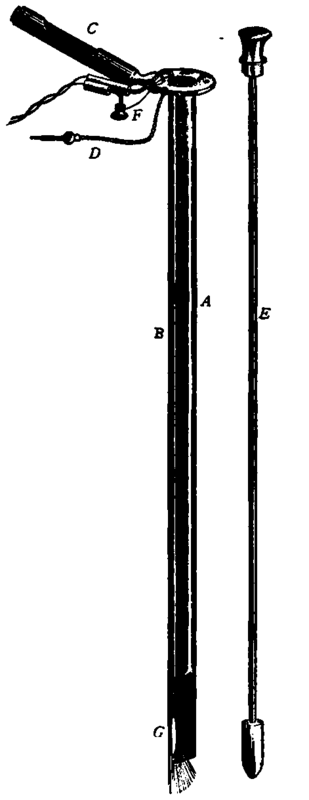
Fig. 5. - The Oesopha-gosoope; lower part partially removed to show its construction. (1/3 natural size).
A, Hollow metal tube.
B, Longitudinal groove.
C, Handle.
D, Plug.
E Obturator.
F. Carrier with wires.
G. Lamp.
1 The carrier can be easily removed with the lamp, thus facilitating thorough cleansing and sterilization of the instrument and any necessary renewal of lamp.
Before introducing the instrument the obturator must be in place, and is held there firmly by means of the plug (D). After the introduction of the instrument this plug is removed and the obturator withdrawn. The wires are connected with an electric battery, and everything is now ready for inspection. The handle (C) facilitates the use of the instrument. I usually practise oesophagoacopy in the sitting posture without any anaesthetic (cocaine spray, etc.). The procedure is not a difficult one, and is done as follows:

Fig. 8. Showing Patient with Oesophagoscope insertal ready for inspection.
Method
The patient sits on a chair which has a back. The instrument (with obturator inserted) is immersed in warm water, and, while depressing the tongue with the left index finger, is held in the right hand like a pen and introduced into the mouth and pharynx of the patient. The latter is now directed to throw his head backward, and the instrument is then pushed down into the oesophagus without exerting any force.
The accompanying drawing (Fig. 6) shows the position of the patient after the introduction of the instrument. Attention must be paid that the lips of the patient are not pressed by the instrument. The obturator is now removed, the connection made, and an inspection may then take place by looking into the tube. At the end of this, the mucous membrane of the oesophagus is plainly visible. If the instrument is slowly withdrawn while looking into it, the whole wall of the oesophagus may thus be inspected.
I have had the oesophagoscope made in three different lengths (35, 40, and 44 cm.) and two thicknesses (1 and 1.5 cm.), which will fulfil various indications. The thicker instrument will be used more especially in the local application of the medicaments, or for the removal of foreign bodies, whereas we would ordinarily get along with the more slender instrument.
Continue to:
My Books

