Chapter I. The Cancer Problem
Description
This section is from the book "Early Detection And Diagnosis Of Cancer", by Walter E. O'Donnell. Also available from Amazon: Early Detection And Diagnosis Of Cancer.
Chapter I. The Cancer Problem
Cancer is truly one of the major public health problems of our times. There were approximately 40 million persons in the United States over 40 years of age in 1935 and about 64 million in 1960, and it is estimated that there will be some 74 million in 1970. This continuing increase in the number of persons in the so-called "cancer age groups" makes it certain that the cancer problem will assume more importance with every passing year.
Cancer is now the second leading cause of death in the United States, accounting for approximately 270,000 deaths in 1961, and this figure is increasing at a rate of over 5,000 deaths each year. The percentage distribution of the major causes of cancer mortality is shown in Fig. 1.
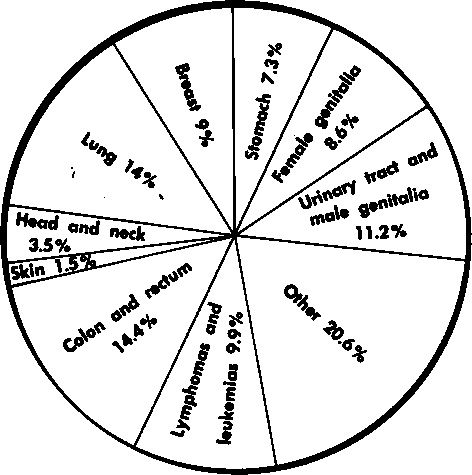
Fig. 1. Estimated 1961 cancer mortality-270,000 deaths, male and female combined.
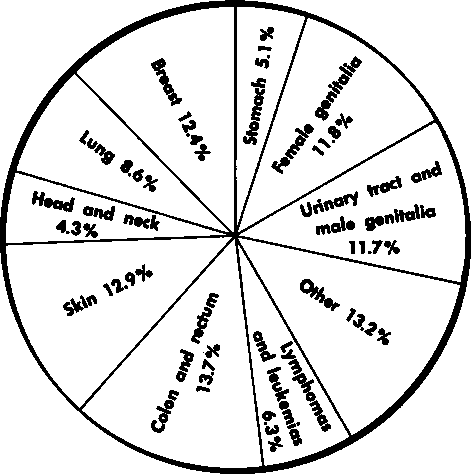
Fig. 2. Estimated 1961 cancer incidence-510,000 new cases, male and female combined.
The real challenge of the problem for the medical profession is underscored by the annual cancer incidence, which was estimated to exceed 500,000 in 1961 (Fig. 2). The American Cancer Society reports that approximately 170,000 of these new cancer patients in 1981 are cured but that an additional 85,000 persons could also be cured merely by the full and timely application of currently available methods of diagnosis without further research or advances in treatment.
The key to the problem is the application of the principles of cancer detection and early diagnosis by physicians throughout the country. This powerful and immediately effective cancer control program has three phases: (1) earlier diagnosis in the symptomatic patient, (2) detection of cancer in the asymptomatic patient, and (3) detection and correction of precancerous conditions for actual cancer prevention.
Earlier Diagnosis In The Symptomatic Patient
The diagnosis of cancer in the patient who has developed suggestive symptoms or signs does not usually present a major problem to the alert practitioner. Once suspicion of this diagnosis has been created, both physician and patient generally are sufficiently motivated to invest the time, expense, and thoughtful attention required to rule the diagnosis in or out. There are, of course, particular situations (singly or in combination), such as those involving an uncooperative patient, an overworked physician, certain characteristically occult neoplasms, or a lesion with highly atypical presenting symptoms or signs, in which the diagnosis may be long delayed or missed entirely. However, presently available methods of investigation, including x-ray, biopsy, cytology, blood studies, and other laboratory aids, suffice to make the diagnosis in about nine out of ten of those persons in whom a major suspicion of cancer exists.
The unfortunate fact is that often the suspicion of cancer is only relatively minor due either to the rather subtle and nonspecific nature of the signs and symptoms or to the patient and physician's lack of awareness of their significance. It is in this area that there still remains room for considerable improvement. Allowing a minor suspicion of cancer to progress to a major one often spells the difference between success and failure in treatment.
Continue to:
My Books

