Chapter VIII. Mobilisation As A Sequel To Massage. 2. Active Movement
Description
This section is from the book "Massage Its Principles And Practice", by James B. Mennell. Also available from Amazon: Massage It's Principles and Practice.
Chapter VIII. Mobilisation As A Sequel To Massage. 2. Active Movement
There is one manoeuvre which can often find a place in our treatment, but which cannot be classed under the heading of "movement." It consists of teaching the patient to contract certain muscles, or groups of muscles, voluntarily without moving any joint as a result of the contraction. For example, the quadriceps can be exercised freely even though the knee be firmly fixed by a splint; the deltoid can be made to contract without any effect on the shoulder-joint. There are two requisites, a little tact and patience on the part of the instructor and perseverance on the part of the patient, if the full benefit is to be reaped. Few things are more injurious to muscular strength than absolute rest; it is surprising how little exercise will maintain it. Even in the absence of joint movement, the performance of the natural function of a muscle - alternate contraction and relaxation - will often suffice, if not to prevent wasting, at least to minimise it and to maintain its vitality. It will also help to maintain intact the muscle-sense on which co-ordinated movement will subsequently rely.
Active movement may be divided into the following groups: -
1. Free movement,
2. Assistive movement,
3. Resistive movement.
1. Free Movement. - We must remember that gravity serves as an effective resistance against which to work, and, if a movement is performed against gravity, we are really performing a concentric movement against resistance; if with gravity, our movement is assisted. Thus it comes about that, in certain positions, assistance may be required if a movement is to be truly "free." In movement of the shoulder, for instance, if the patient is standing, exercise with the weight and pulley may mean that movements of abduction and adduction are almost "free" because the weights counteract the weight of the limb during the movements. The so-called "free" abduction is a movement against the resistance of gravity if the patient is upright, while adduction is a movement assisted by gravity. True "free" movement is, therefore, excessively rare; and the division of movement into "free" and "assistive" is arbitrary. It is useful, nevertheless, as it serves to remind us that active movement may be "active," even though only performed with assistance. Free flexion and extension of the fingers is best performed with the hand supported on its ulnar border, the forearm being held mid-way between pronation and supination. For the exercise of free adduction and abduction the hand should be placed flat upon a table, and the fingers are then separated and approximated. It is sometimes of service to keep them rigid by means of light posterior splints.

Fig. 41. - To show the position for free rotation of the forearm, the patient being recumbent.
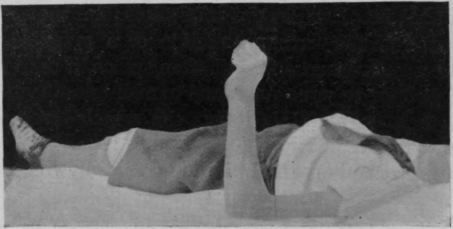
Fig. 42. - To show the same position as in Fig. 41, free movement having been performed from almost full supination to full pronation.
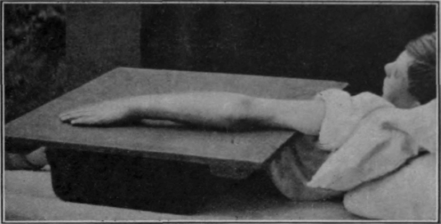
Fig. 43. - To show the starting position for free flexion of the elbow. This is also the end position of free extension.
The forearm being supported in this position with the hand hanging free is the correct attitude in which to perform free flexion and extension of the wrist.

Fig. 44. - To show the starting position for free extension of the elbow. This is also the end position of free flexion.
Free rotation is performed starting from the same position, the hand being supported or not, according to the nature of the case. Better still, the patient lies flat on his back, the posterior aspect of the arm rests on the couch, and the forearm is kept vertical by flexion of the elbow to a right angle (see Figs. 41 and 42).
Free flexion and extension of the forearm is best performed with the patient recumbent, the inner side of the arm and the elbow being fully supported and the hand moved up and down over the chest (see Figs. 43 and 44). The movement is almost free through an angle of 15 degrees in either direction if the forearm is kept vertical. As an alternative method, if shoulder movement will permit, the patient sits beside a table in such a position that its surface is on a level with the axilla.
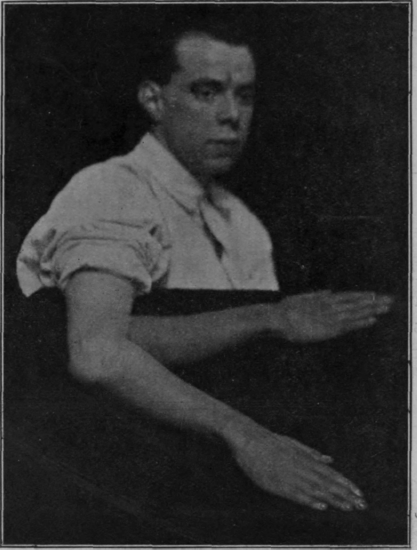
Fig. 45. - To show flexion and extension of the elbow while the limb rests on an adjustable board. When the board is horizontal the movement is free except for the resistance due to friction. As its outer edge is depressed flexion is resisted by gravity and extension is assisted.
The whole arm then rests upon the top of the table while flexion and extension are performed (see Fig. 45).
Free movement of the shoulder entails the supporting, by one means or another, of the weight of the forearm and hand.
Continue to:
My Books

