Chapter XX. Re-Education In Walking
Description
This section is from the book "Massage Its Principles And Practice", by James B. Mennell. Also available from Amazon: Massage It's Principles and Practice.
Chapter XX. Re-Education In Walking
Re-education in walking is a special art which calls for the exercise of great skill, but the reward is directly proportionate to the amount displayed.
Muscle re-education should begin before any joint can be moved, and while, if necessary, the limb is still encased in plaster. The patient is taught to contract and exercise each muscle or muscle group in turn in the manner already described for the treatment of splint or sling atrophy of the arm.
Too much importance cannot he attached to ensuring the return of co-ordination. After any lengthy period of inaction, from whatever cause, this power is impaired, and after injury the impairment is more marked. Every movement is the result of muscular contraction combined with relaxation of the antagonistic muscles. In walking, not only is this true, but the efficient working of one muscle is dependent on similar capacity in many others, some of them very remote. Even the placing of both hands in the trouser pockets has a marked effect on the general co-ordination of the body during locomotion. It is easy, therefore, to realise that marked weakness of one muscle, or of a group of muscles more intimately concerned with the movements of the lower limbs, will greatly militate against perfect co-ordination. Yet after injury of any sort there is a tendency for muscular wasting to follow, perhaps from disuse only, perhaps as a result of injury inflicted directly on the muscle, its nerve or vascular supply, or even on account of reflex action excited by injury to a joint whose movement is controlled by the muscle. Not only is the wasting significant of weakness, but a wasted muscle invariably requires a longer latent period to pass than does a normal muscle between the receipt of stimulus via its nerve and its subsequent response. This often holds good even if no obvious wasting can be detected. Thus it is impossible for a muscle which has been injured directly or indirectly to react normally to the impulses it receives, but the uninjured muscles concerned continue to do so. The inevitable result is loss of co-ordination.
Our first business, then, is to ensure the restoration of coordination in existing circumstances - or, in other words, to teach the muscles which have suffered least, or not at all, to adapt their contraction to suit that of their less fortunate fellows - and then to continue the process by educating the sound limb to adapt itself to any little vagaries of the injured limb.
The most simple movements should precede the more complicated, and so the first stage, whenever possible, should be to encourage the patient to swing the feet to and fro alternately over the side of the bed or couch. Often the first instinct of the patient is to swing them together, but this should be prohibited until the alternate swing has become quite natural, free from all rigidity and stiffness, until, in fact, a "loose swing" has been attained. Perfection cannot be attained until the movement is effortless: hence the necessity of starting with a swing through a range of minute amplitude. The range is very gradually increased. Then swinging together may be prescribed, followed by the performance of the two exercises alternately. These exercises must be continued till their performance is quite natural and free from all effort. If the instinct to swing the legs together is encouraged at the start instead of the alternate swing, "looseness" in movement is not so readily acquired, and the patient is liable to resent the persevering effort of the masseur to secure perfection in the alternate leg-swinging.
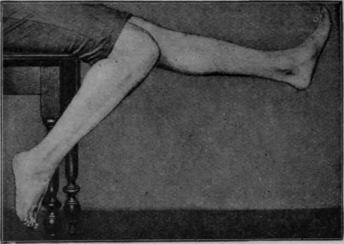
Fig. 104. - The final swinging exercise while sitting. Note the plantar-flexion of the ankle with flexion of the knee, and dorsi-flexion with extension of the knee.
The swinging exercise may be advanced a stage by being performed with regular alterations in the rhythm. At the same time opportunity arises for increasing the strength of weakened muscle groups by calling upon them to contract to the full extent of their power. The best plan is for the patient to swing the feet alternately three or four times and then to hold the sound leg out straight while counting three slowly. The swinging is continued and the weakened leg is held in the same position for the same time. The length of time is gradually increased. The process is repeated, but now the cessation of movement takes place in the flexed position. Finally the movement is checked and contraction held with one knee bent and the other straight (see Fig. 104). The next stage is to educate ankles and toes to co-operate in the "swing." As each leg swings forwards in turn the ankle and toes are dorsi-flexed; as it swings back they plantar-flex. By the addition of slight hip movements the patient is now able to perform full "bicycling" movements in the air.
Continue to:
My Books

