Re-Education In Walking. Part 2
Description
This section is from the book "Massage Its Principles And Practice", by James B. Mennell. Also available from Amazon: Massage It's Principles and Practice.
Re-Education In Walking. Part 2
Two exercises can then be added. The patient stands on the sound leg between two chairs placed back to back and swings the injured leg to and fro. At first this will be done with a stiff knee and ankle, but gradually the muscles will be able to relax and the knee will bend as the thigh extends and the ankle will plantar-flex (see Fig. 105). On swinging forward, the knee will straighten and the ankle dorsi-flex (see Fig. 106). This is the natural movement of walking, and it may require close attention to see that it is efficiently carried out. It will be noticed that in this exercise alone a different combination of movement is required when treating a patient by relaxed or by active exercises (cf. p. 69). This is because the ankle movement in walking is the only natural movement that is performed in such a manner that the musculature is, as it were, at a disadvantage. Hence the natural "trick" of ankle movement in walking is very readily lost and supplanted by purely "natural" movement. After a few swings the patient sits down and places both feet flat on the floor with the knees extended to slightly more than a right angle. The toes of the sound foot are then raised from the floor and are lowered again while the heel rests on the ground (cf. Fig. 109). The foot of the injured limb follows suit. Flexion of the knee progresses until a point is reached when it is impossible to raise the toes, and then the heels are raised alternately while the toes rest on the floor (see Fig. 107). As the feet are drawn further and further under the chair the movement becomes more limited till finally little or no movement can be obtained, but the toes and ankle can still be exercised together (see Fig. 108). Once more the knees are extended slightly till the soles of the feet rest easily on the ground. The two exercises are then combined, and the patient executes a species of "clog-dance" (see Fig. 109) - right toe, left toe, right heel, left heel, each tapping the ground in turn. The sense of hearing helps to maintain the rhythm. It will then be found that all the movements of ankle and toes which form a part of natural walking have been performed, though no weight has been placed upon the foot. The exercises can be made more severe from day to day by increasing the frequency of the movements, by the gradual alteration of the position of the feet, and by holding them in the extremes of movement while counting. Between the exercises, unless contra-indicated (as, for instance, after a recent fracture of the internal malleolus), the patient is taught to rest with the legs crossed and the feet resting on their outer borders. He is then told to claw with the toes and to try to shape the foot as would do a monkey trying to climb up a pole. Having learnt to "claw" properly, he is told to maintain the position while counting (see Fig. 110).

Fig. 105. - Swinging the leg while standing. Note plantar-flexion of the ankle and flexion of the knee. The patient is shown supporting himself by a chair placed in front of him for clearness in reproduction.

Fig. 106. - Second stage in swinging the knee. Note dorsi-flexion with extension of the knee.
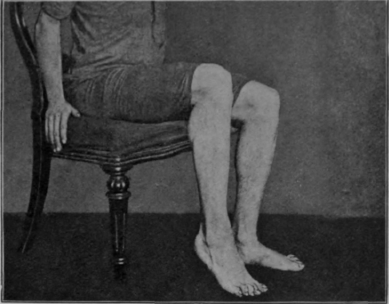
Fig. 107. - Second stage of the first sitting exercise. The heel is raised and lowered.
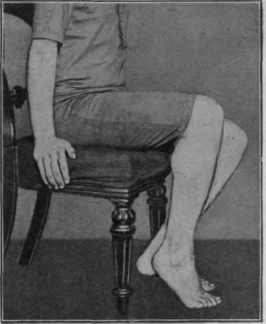
Fig. 108. - The final stage in the first sitting exercise. The heels cannot reach the ground.
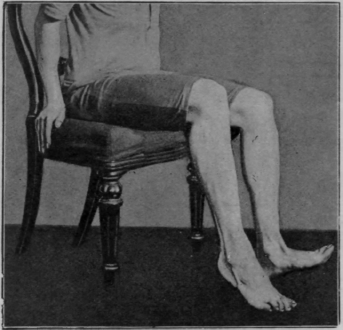
Fig. 109. - The first two sitting exercises in the re-education of walking combined. The toes are raised and lowered, alternating with similar action of the heels. The result is the "species of clog-dance" referred to in the text.

Fig. 110. - To illustrate the "clawing" exercise while sitting.
As the rapidity of the exercises increases more and more weight is gradually placed upon the feet, but so far only a negligible amount has been so placed compared with the weight of the body, and the main object hitherto has been to accustom the limbs to move in unison, and to train the various muscle groups in the injured limb to co-operate with one another. Meanwhile it is possible to continue to build up the strength of the weakened muscle groups by perseverance with the original exercise of holding contraction, while counting without actual joint movement, and by paying special attention to holding the contraction during certain movements of those muscles which are weakened.
Exercises on the sliding-seat follow. They should begin with the foot-piece loose and the supporting bar at the lowest level. Day by day the bar is raised, and the elevation of the inclined plane is thus increased. When the exercise can be performed freely with the elevation at its maximum, considerable pressure is exerted on the foot. Probably the patient will do most of the work with the sound leg: this does not matter, as it will tire and the injured limb will then be called upon instinctively to play its part. Moreover, all the time hip, knee, and ankle are acting in unison. The masseur can often assist greatly by supporting the knee, or even by gentle kneading during the limits of movement if flexion is deficient. Extension can be aided by pressure on the knee while kneading the hamstrings. The great point is to see that the seat is driven back to the limit. For emphasis it is well to repeat that it is the power of maintenance of full extension which is, above all, required to maintain the stability of a knee-joint.
The bar is then lowered and the foot-piece is fixed in the position best adapted to secure the performance of the particular movement which happens to be most limited. The more nearly the foot-piece approaches the horizontal the more full does flexion of the knee become. The bar is raised gradually as the days pass.
Assistance to all these movements can be given by various combinations with the weight and pulley. The lowest pulley can be utilised by holding the cords in the hands; thus rowing is more nearly simulated. The rope over the top pulley can be attached round the knee, but this device is not used very frequently. The patient can be taught to assist the movement by keeping the hands on the knees and pressing down, or under the knees and pulling up (cf. Figs. 50 and 51, p. 104). Otherwise the hands should grasp the seat or rails.
Continue to:
My Books

