I. Passive Movement. Part 3
Description
This section is from the book "Massage Its Principles And Practice", by James B. Mennell. Also available from Amazon: Massage It's Principles and Practice.
I. Passive Movement. Part 3
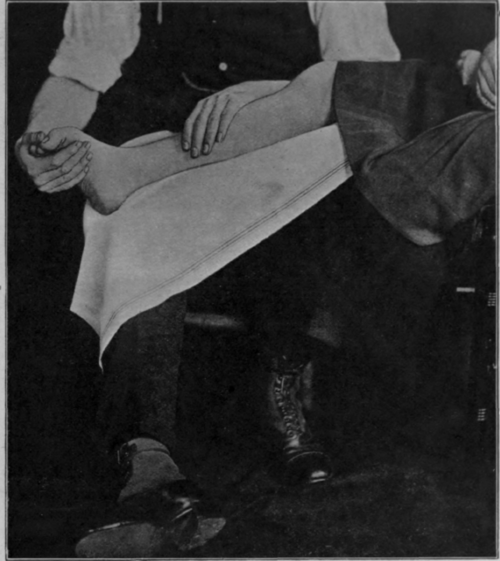
Fig. 30. - To show flexion of the toes with dorsi-flexion of the ankle. Note the knee is bent.

Fig. 31. - To show extension of the toes with relative plantar flexion of the ankle. Note the knee is slightly extended as compared with Fig. 30.

Fig. 32. - To show most useful position for mobilisation of the knee. Note the "play" of the masseur's feet when comparing these figures and Nos. 33 and 34.
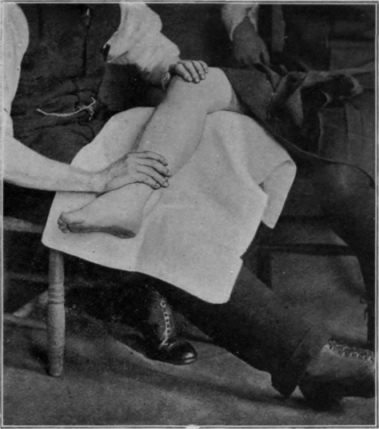
Fig. 33. - To contrast with Fig. 32. The control in these positions is perfect.

Fig. 34. - Another method of securing flexion of the knee, the thigh being fixed. The masseur should be standing further to the right at the side of the patient, but this could not be shown in the photograph.
Mobilisation of the phalanges of the hand is frequently mismanaged, with the result that a mild degree of tendon insufficiency is left undiagnosed and untreated. It often happens that after injury a patient is told to keep the fingers supple by movement. The patient obeys; but, owing to lack of instruction, movement takes place only at the interphalangeal joints. The range of movement at the metacarpo-phalangeal joints then becomes limited and the impairment of movement is most disastrous. Unless there is obvious impediment to such a procedure, the technique of mobilisation for the fingers is to extend fully each joint in turn, commencing with the distal interphalangeal joint. Flexion should then be undertaken by bending down to its full extent the metacarpo-phalangeal joint; the first interphalangeal joint is next dealt with, but towards the limit of its flexion that of the metacarpo-phalangeal joint must be slightly relaxed. As we continue this relaxation slowly, the terminal interphalangeal joint is fully bent and is maintained in this position while the metacarpo-phalangeal joint is straightened. The proximal interphalangeal joint is then straightened, and finally the distal (see Figs. 38, 39, and 40).

Fig. 35. - To show position for administering movement to the hip The same position is also of service when mobilising the knee.

Fig. 36. - To show the grip for lateralising the inferior radioulnar joint.
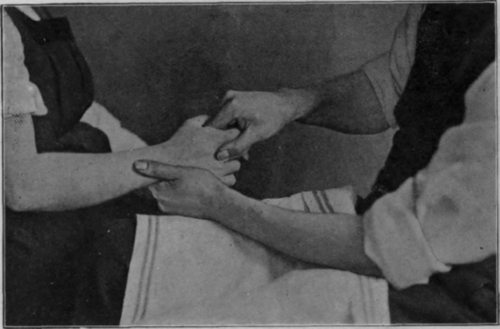
Fig. 37. - To show the grip for loosening the joints between the bases of the second and third metacarpals.
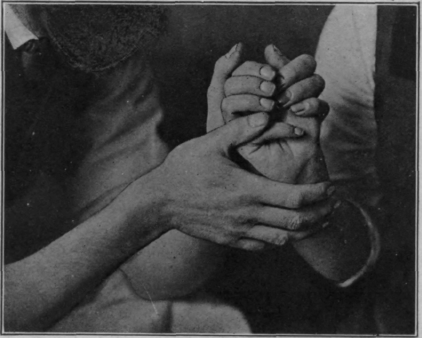
Fig. 38. - First position in performing flexion of a single finger. The metacarpo-phalangeal joint is fully flexed. Note the extension of the wrist. Either the index finger or the thumb may be used to perform the movement. (For further details of technique, see Chap. XVII.)

Fig. 39. - Second position in performing flexion of the fingers. The proximal interphalangeal joint is fully flexed, the metacarpo-phalangeal has been slightly extended.
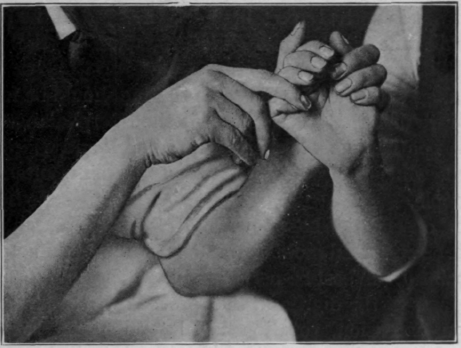
Fig. 40. - Third position in performing flexion of the fingers. The distal interphalangeal joint is fully flexed as well as the proximal. To effect this the metacarpo-phalangeal joint has been fully extended.
It is essential to bear in mind that flexion and extension at all the finger joints is not a pure hinge movement. Thus, during flexion of the proximal phalanx on the metacarpal, the base of the former performs a distinct gliding movement over the head of the latter. Forcible movement performed with disregard of this important fact simply inflicts a severe strain on the posterior ligaments, and the result is often disastrous. When there is considerable stiffness in the finger-joints the positions shown in Figs. 38 - 40 are not ideal for the administration of forced (or assistive) movement. The alteration required (too difficult to show in an illustration) is that the masseur's left hand should be engaged, not only in giving support, but in actively pressing back the head of the proximal bone while the right hand glides the base of the phalanx over it.
Continue to:
My Books

