I. Passive Movement. Part 2
Description
This section is from the book "Massage Its Principles And Practice", by James B. Mennell. Also available from Amazon: Massage It's Principles and Practice.
I. Passive Movement. Part 2
Fig. 23. - To show how the forearm should be carried across the front of the chest (as if it were resting on an adjustable sling) when changing from supination to pronation.
Flexion of the forearm is most easily performed if the elbow is pressed backwards at the same time, i.e., during extension of the shoulder: extension of the elbow is performed while the shoulder is flexed and the arm carried forwards (see Figs. 25, 26, 27, and 28).

Fig. 24. - To show pronation of forearm with extension of elbow. The positions should be compared with those shown in the two previous figures.
Abduction of the arm is combined with flexion of the elbow: during adduction the elbow should be somewhat extended (see Fig. 29).
Flexion of the toes should be combined with dorsi-flexion of the ankle: extension with plantar flexion (see Figs. 30 and 31).
Plantar flexion of the ankle calls for extension of the knee, though the knee should be kept slightly flexed even when the ankle movement is at its extreme: dorsi-flexion requires increasing flexion of the knee.
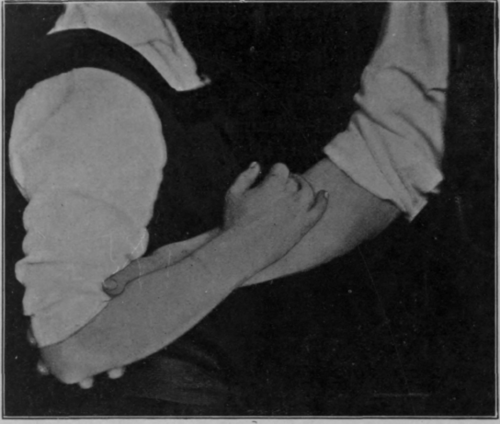
Fig. 25. - To show position for all early relaxed movements of elbow or shoulder. Note the combined flexion of elbow, extension of shoulder and supination of wrist.
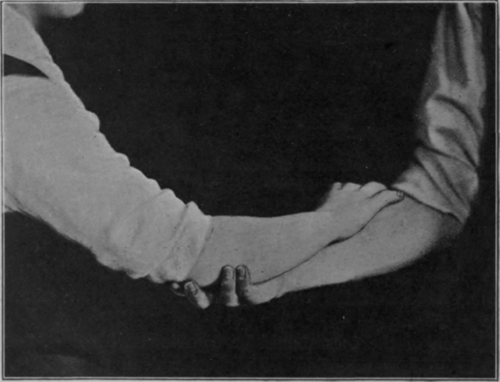
Fig. 26. - Note the position at each joint in contrast to those shown in Fig. 25.
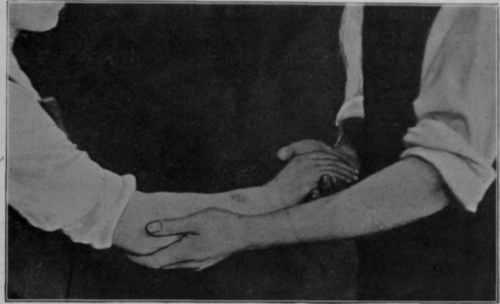
Fig. 27. - To show another position that may be used during later stages of treatment for mobilisation of shoulder and elbow, the latter being extended.
Flexion of the knee should be combined with flexion of the hip: extension of the knee with extension of the hip (see Figs. 32, 33, 34, and 35). Adduction and abduction of the hip is best performed with knee and ankle semi-flexed: its rotation requires alternate flexion and extension of the knee, flexion accompanying that part of the movement when the hip is most flexed, and extension of the knee the part when the hip is most extended (see Fig. 35).

Fig. 28. - The same as Fig. 27, showing elbow flexed. Note again the rotation of forearm.
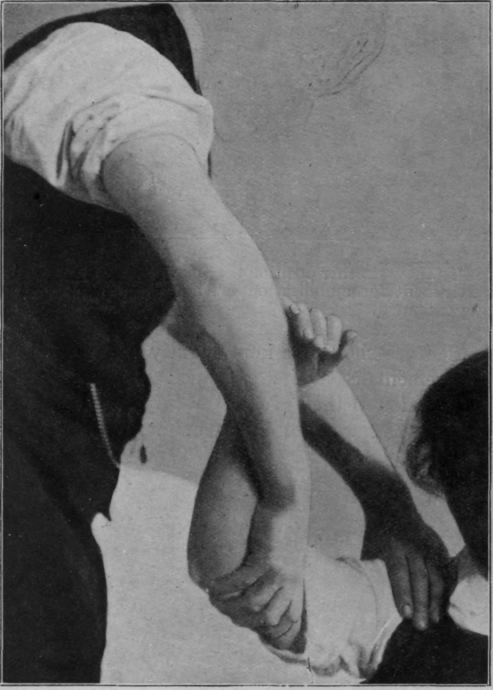
Fig. 29. - To show one position in administering circumduction of shoulder. The support given by the masseur's right hand and arm is identical with that shown in Figs. 25 and 26.
It is almost impossible to administer a dose of relaxed movement to the lower limb except in the presence of some degree of flexion of the knee.
In all movements of the knee the slight rotatory movement which is possible must be kept in mind and be administered in flexion. In the same way, all interphalangeal joints are capable of lateral movement, but in a slightly flexed position: the inferior radio-ulnar joint frequently calls for anteroposterior mobilisation, most freely obtained with the forearm between pronation and supination, the amount lessening towards the two extremes of rotation (see Fig. 36). The joints at the bases of metacarpals and metatarsals are frequently overlooked, but they should all receive their dose of movement (see Fig. 37). The most important of all the joints at the bases of the metacarpals is of course that at the base of the first. It must always be kept in mind that the power of opposition of the thumb is the one vitally essential movement in the whole hand. Without it the function of the upper extremity is largely reduced to impotence for most of the ordinary usages of life. It is well, however, to remember that fixation of the metacarpo-phalangeal joint of the annularis in a straight line is a crippling deformity of great severity. The existence of impediment to movement in these joints - often quite easy to correct - is a source of great weakness to the grip, or may be the cause of otherwise unaccountable limping due to pain in the foot. Though no true joint exists, mobilisation should be administered to the heads of metatarsals and metacarpals. It is often surprising to find how readily movement returns to fingers which are apparently quite stiff in extension, if the heads of the metacarpals are loosened until a palmar concave arch is visible. If the fingers are fixed and bent, the first step in treatment should be to flatten this arch. The same applies to manipulation of the foot. It is difficult to mobilise the carpal joints, but not so the tarsal joints. These should always receive care and attention, especially the astragalo-scaphoid and calcaneo-cuboid joints. A firm grip is taken of the foot on either side of the joints, and an "up-and-down" movement is imparted, combined with an attempt to perform rotation of the anterior part of the foot upon the posterior.
Continue to:
My Books

