The Treatment Of Deformities. Part 4
Description
This section is from the book "Massage Its Principles And Practice", by James B. Mennell. Also available from Amazon: Massage It's Principles and Practice.
The Treatment Of Deformities. Part 4

Fig. 151. - To show position for administering resistive exercises in metatarsalgia. The patient "claws" with the toes while the hand supports the sole behind the metatarsal heads, thus helping to restore the arch from below.

Fig. 152. - Showing an alternative exercise for metatarsalgia. The patient dorsi-flexes the ankle and "claws" with the toes, the hand in this case assisting in moulding the arch from above.
Valuable as the means already considered may be, they must be considered solely as adjuvants. The main remedial agent is muscle-training. A start should be given with manual training. The ball of the thumb is placed on the sole of the foot in such a position that it fits exactly into the concavity formed by the heads of the metatarsals. If the hand is too far forward - a common fault - it will, by its pressure, cause pain. The patient is taught to "claw" with his toes while the dorsi-flexion of the ankle is secured by the masseur's hand. In this way the arch is restored and the muscles are trained to maintain it. In this position, by attempting to "claw" with the toes, the lumbricals are brought into effective action (see Figs. 151 and 152). This exercise may alternate with a second, namely, to mould the arch with the hand placed over the dorsum of the foot so as to hold it in shape while the foot is plantar-flexed. The patient then dorsi-flexes the foot against the masseur's resistance, maintaining the full "clawing" action while he does so.

Fig. 153. - Capt. James Patterson's "footboard." It is made of wood, the dimensions being 9 1/2 ins. by 5 ins. by 1 in.
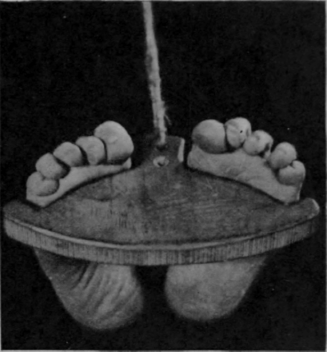
Fig. 154. - Capt Patterson's "footboard" in use. The cord is held in the patient's hands and he exerts the necessary tension. The knees are kept rigidly in full extension and the ankles in dorsi-flexion.
As soon as the patient has gained elementary proficiency he may be promoted to the use of Capt. Patterson's foot-board. This is shown in Fig. 153, and in use in Fig. 154. It serves the same purpose as the first of the exercises described above; but it can be used by the patient without assistance, and he regulates his own resistance, usually far more efficiently than can the masseur, as soon as he has learnt the "trick."
The next thing to be learnt is to pick up a large marble, then a golf-ball (see Fig. 155), and finally, a tennis-ball with the foot (see Figs. 156 and 157). The ball is placed on the floor well behind the ball of the foot, and the latter is then slowly pulled backwards while the patient "claws" down upon it till he succeeds in grasping it firmly enough to pick it up. It is when attempting to pick up the larger balls that the adductor transversus is brought prominently into action.

Fig. 155. - The patient has picked up a golf ball with his toes.
Other valuable exercises are easily devised, such as learning to balance while standing on a small football; climbing a ladder barefooted with the feet inverted, the rungs being just behind the metatarsal heads, and picking up various objects between the soles of the two feet. Free-standing exercises for patients with claw-foot tendencies should all partake of the "lunge" position variety. Anything that tends to stretch the tendo achillis and to push up the metatarsal arch may be used with advantage (see also Chapter XX (Re-Education In Walking)., p. 284).
The treatment of hallux rigidus is often most disappointing. This is not to be wondered at when we remember that, even under an anaesthetic, mobility cannot be restored by sheer force. In early cases, however, an attempt may be made to help. The foot should be thoroughly heated and firm longitudinal tension should first be applied. Then full lateral mobility should be secured and, finally, any rotation which may be Deformities of the lower extremity other than those mentioned rarely find their way into the massage-room for treatment. Occasionally a case of hysterical spasm may be found.

Fig. 156. - To show the grip required when picking up a tennis-ball with the toes. (Cf. Fig. 157.) possible before an attempt is made to secure dorsi-flexion. The longitudinal tension should be applied throughout and any marked reaction, shown usually by increased sensitiveness or decreased mobility, must be regarded as definite indication that we have attempted too much. Unless improvement is manifest in a few days, it is usually better to regard the case as hopeless and forthwith consider the pros and cons of operation.
If there is no obvious and very definite sign of immediate improvement, the sooner treatment by massage is abandoned the better for all concerned. Paralytic deformities call for treatment on the lines laid down respectively for that of flaccid and spastic paralysis.
Spinal deformities rarely need massage treatment at all, though it may be useful occasionally to "space" a few minutes' treatment between the various exercises. The main objective is to provide a sort of general "refresher."

Fig. 157. - A second view showing the grip required when picking up a tennis-ball with the toes.
Continue to:
My Books

