The Treatment Of Neuralgia And Neuritis. Part 4
Description
This section is from the book "Massage Its Principles And Practice", by James B. Mennell. Also available from Amazon: Massage It's Principles and Practice.
The Treatment Of Neuralgia And Neuritis. Part 4
In cases of long standing nothing can compare with massage as a remedial agent. After operation, or sudden stretching, adhesions will almost inevitably re-form, whereas slow, gradual stretching by manipulation should inflict no damage which entails repair in the shape of re-formation. On the other hand, if any attempt is made to hasten recovery unduly, actual rupture of the adhesions may take place; and, in that case, the continued vigorous manipulation of the structures, which have been subjected to this recent injury, may well aggravate the condition. Attention to the law of treatment, that all points which are hypersensitive are the last that should receive attention, will avert catastrophe.
Treatment, therefore, should begin on the front of the thigh. The quadriceps should be kneaded gently, and should then receive a thorough shaking as soon as the condition permits. Treatment of the calf on similar lines follows. Then, and not till then, may "local" treatment of the nerve begin. The preliminary stages may be passed through during the first twenty minutes of treatment, or may require as many days. The same routine should be followed on the back of the thigh while the foot is well elevated on a pillow. As the condition improves the elevation is decreased day by day till the limb rests in the horizontal plane. The patient now lies close to the edge of the bed, and the foot is slowly lowered over the side, while the kneading and shaking continue. As soon as an angle of some 45 degrees with the horizontal has been reached, treatment is more simply conducted with the patient supine. The knee is flexed and raised till the thigh is perpendicular, and thereafter full flexion of the thigh on the trunk can be effected, the continuance of the kneading and shaking assisting the process. The knee is then straightened by slow stages, and finally the foot is dorsi-flexed (see Figs. 145 to 147). By following some such scheme as the above, a case of many months' standing may yield to treatment in a few weeks or even days. To hurry is to court disaster. Pseudo-sciatica, due to "sacro-iliac strain," is considered in the following chapter.
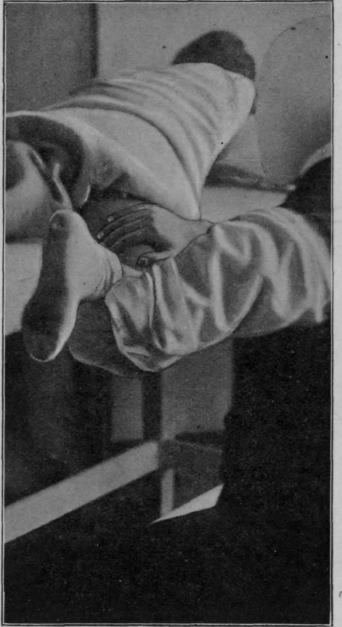
Fig. 145. - To show position for treatment of a case of sciatica, the "cure" being well advanced.
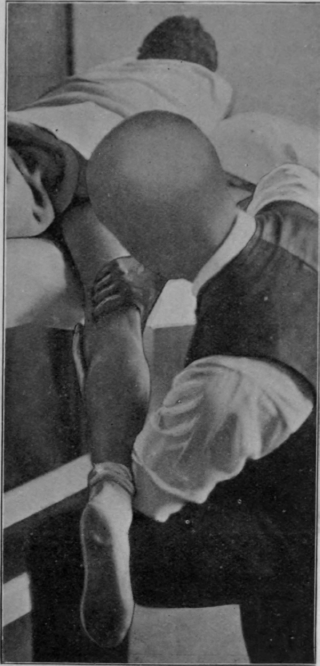
Fig. 146. - The end of the movement shown in Fig. 145.
When it is evident that any adhesions which may have been present are yielding to treatment, search should be made throughout the whole course of the nerve for any tender points or for "nodal" formations. These may be subjected to frictions, but treatment must start very gently, and the increase of pressure must be graduated with the utmost nicety. It should always be remembered in this connection that symptoms of subacute sciatica may be due to a fibrositis of the gluteus maxi-mus and medius. Tender points over these muscles should therefore be sought out and treated.
All other forms of neuritis of long standing should be treated on similar lines, as, for example, occipital and supra-orbital neuritis. Here vibration may replace shaking.
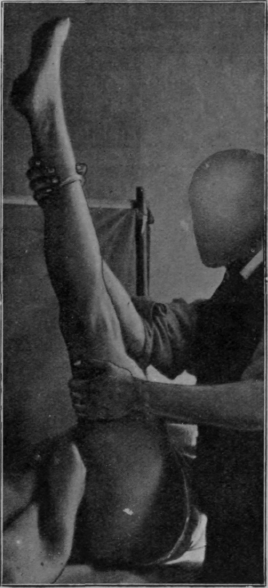
Fig. 147. - To show how the foot naturally passes into plantar flexion when the hip-joint is flexed, the knee being fully extended. Dorsi-flexion of the ankle adds materially to the stretching of all structures on the back of the limb.1
1 Prof. M. L. Rimbaud has described a frequent sign of sciatic nerve trouble. This is partial obliteration of the hollows on either side of the tendo achillis (effacement retromalleolaire). It is particularly obvious if the internal popliteal element has been involved in injury or by disease, and is probably due to loss of tone in the muscles of the calf.
The cause of the pain of coccydynia is unknown. It may be due to a pressure neuritis affecting the small nerve filaments which lie in the periosteum. A chronic periostitis may cause the neuritis. Or, again, it may be due to adhesions in or around the joints. Whatever may be the cause, gradual approach with the vibrator will often cure, even when all other remedies have been tried and found wanting.
Before any other line of treatment is considered a rectal examination should be made, and each joint of the coccygeal region should be firmly manipulated throughout its full range. A firm grip can be secured between the index finger in the bowel and the thumb outside. Flexion and extension are the main movements, but a small amount of rotation is possible and must not be overlooked. Severe and long-standing cases can often be cured permanently at one sitting by skilled manipulation. In other cases the symptoms may return, but manipulation again secures relief for a considerable time.
In the acute stage of sciatica and of other forms of neuritis the advisability of using massage is a moot point. The trouble is inflammatory, and in the presence of acute inflammation massage is contra-indicated. But the cause of the inflammation is rarely due to any micro-organism, and so the danger of inflicting injury on the patient by massage is more imaginary than real. In fact, it may be possible at times to abort an attack, if treatment is administered within a few hours of its onset. Surface stroking of the anterior aspect of the whole limb should be succeeded by deep stroking and by kneading in turn as each becomes tolerable. The patient then assumes the prone position, and the process is repeated on the back of the limb. Relief must be progressive throughout, or treatment must be abandoned.
If the attack has lasted more than twenty-four hours before the first dose of massage is given, it will probably be found impossible to administer this full treatment, but all the manipulations which are possible without removing the patient from the supine position can be performed, and thus the circulation of the whole limb can be improved. This will hasten the removal of the cause of the irritation. Later on a more complete treatment can be administered.
Brachial neuritis, for some reason, does not yield successfully to treatment to the same extent as sciatica. Whenever treatment fails to relieve, absolute rest is indicated. But even so massage can help. It has been proved on countless occasions that abdominal massage hastens the elimination of waste products; and, whenever it is possible to procure it for them, no sufferers from neuritis should be deprived of this means of assistance.
Dr. Goldthwait, of Boston, Mass., pointed out to me the importance of taking into consideration the value of postural treatment for this type of case. When the head is carried with a forward stoop and the shoulders are held well back, correction of posture will often be found to afford relief. The chance of being able to relieve by manipulation of the joints between the cervical vertebrae will be considered in the next chapter.
Continue to:
My Books

