The Use Of Apparatus For Exercise. Part 2
Description
This section is from the book "Massage Its Principles And Practice", by James B. Mennell. Also available from Amazon: Massage It's Principles and Practice.
The Use Of Apparatus For Exercise. Part 2
Few of those who are interested in massage work will fail to know the fame of Wharton Hood. His reputation for being able to restore function to limbs which seemed doomed to permanent weakness was very great; and yet his remedial agents were almost entirely confined to movements under an anaesthetic and subsequent exercise of some form or other with a weight and pulley apparatus. Some of his original apparatus is in use at the Special Surgical Hospital, Shepherd's Bush, and is of the most simple character. With this exception almost all the apparatus used in this hospital was built on the premises by Mr. Hobbs, carpenter to the Hammersmith Infirmary, according to the plans and directions of the author.

Fig. 55. - To show how the exercise depicted in Fig. 54 can become a resistive exercise to the extensors of the hip.
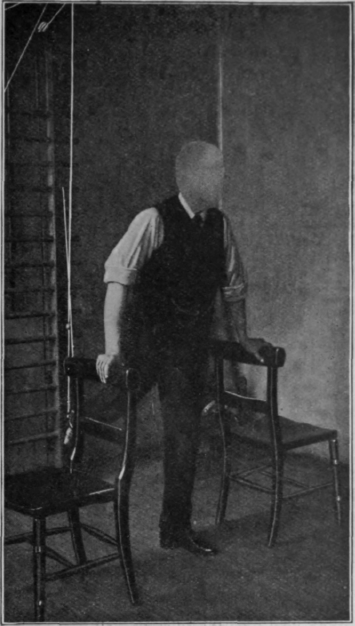
Fig. 56. - To show resistive exercise for the flexors of the hip. The extensors receive assistive exercise, and there is also some resistive exercise given to the quadriceps.
The main structure is depicted in the appendix. Though rather more complicated than Wharton Hood's apparatus, it remains perfectly simple, and the additions were made chiefly to meet the special requirements of a military hospital. An attempt will be made to indicate the exercises that are suitable for various conditions, when later on we come to deal with each condition in turn. There are, however, certain laws which apply to all exercises.
The main point to remember in prescribing exercises is that the dose must be steadily progressive.
As an example let us consider the scheme for restoring a leg, the muscles of which are wasted by disuse - let us say after an attack of typhoid, so as to exclude the necessity of considering any particular joint or muscle-group.

Fig. 57. - To show how the same exercise as that depicted in Fig. 56 can become a full resistive exercise to the extensors of the knee as well as to the flexors of the hip.
When his course of bed-gymnastics has been completed and he is able to get down to the massage-room, the patient starts with exercises on the sliding-seat with the rails practically horizontal. He may even have to assist flexion by the use of his hands under the rails or by the aid of the floor pulley and weight (see Fig. 49). Day by day the inclination of the rail is increased, the foot-piece being left loose. When the inclination can be increased no further, it is reduced and the footpiece is fixed. The inclination is then gradually increased to its maximum (see Figs. 50 and 51).
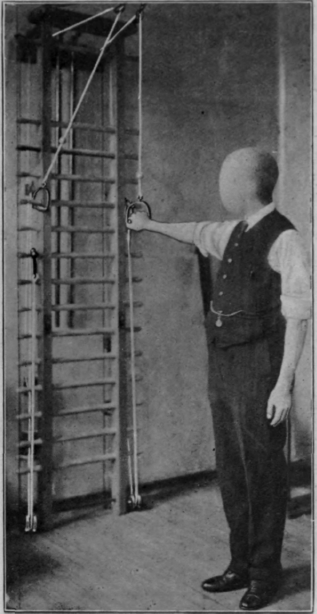
Fig. 58. - Showing "assistive" exercise of the acromial part of the deltoid. Note the patient stands to "attention."
The next stage is exercise with the weight and pulley in the sitting position (see Figs. 52 and 53), then in the standing position (see Figs. 54 to 57). As it is possible with pulleys at three different levels to devise eighteen varieties of movement, each capable of two or three minor modifications, and all being open to at least six alterations in the weights used, it is obvious that three or four weeks can be passed with some daily addition or alteration to mark the daily progress, should such frequent change be deemed of advantage from the psychological point of view. From the purely physical standpoint it would probably serve to make several additions at once, say twice a week. Then, if the patient tires of this form of exercise, an ever-increasing portion can be replaced by exercises on the ladder.
The aim of the prescriber should be to make the alterations so trivial that the patient's muscles fail to recognise that extra strain is being put upon them, while his mind is able to note the changes that mark his progress. At the same time the alterations should be so frequent that an ever-increasing amount of exercise is performed.
Another method of recording progress, say after injury to a knee, is to mark on the rail the position to which the sliding-seat can be moved the first day. Every subsequent day an attempt is made to advance the seat, say half an inch. In a week perhaps the seat has advanced three inches, which entails a considerable amount of extra flexion in the knee-joint. Often this fact will pass unnoticed by the patient, whose attention is fixed on two small marks under his sliding-seat.
Another useful, but little-used, scheme for assisting the return of movement in a joint which has become stiff is to encourage the patient to perform some exercise with the weight and pulley or on the sliding-seat, and to assist the movement by manipulation round or near the joint at the same time. It is often of the greatest value to knead the structures which become tense as the limits of movement are reached.
In devising a scheme of exercises, not only has a steady progress to be arranged, but it is essential to make sure that we know exactly what it is we want to exercise, and to lay our plans accordingly. If a muscle, e.g., the acromial portion of the deltoid, is to be exercised to its full extent, the correct plan of campaign is to ensure that it can relax and contract freely. With this object in view it is not wise to start by making it contract against resistance, but with assistance. Hence the first exercise with the weight and pulley is to allow the weight to abduct the arm to its full extent without any exertion on the part of the patient, while the adductors are exercised in elevating the weight during the return of the arm to the side (see Fig. 58). Although the deltoid is called upon to do no work whatever so far, its fibres are none the less shortening and lengthening with each movement. The weights are then reduced, so that to perform the movement the deltoid has to assist in raising the weight of the arm against gravity. When this can be done freely without the use of weights at all, the patient turns completely round and the weights are once more increased so as to assist adduction while resisting abduction (see Fig.59). The patient during abduction is now experiencing concentric resistive exercise in his deltoid and excentric during adduction. Moreover, the addition of weight now increases the vigour of the exercise for the deltoid, while in the first position decrease in the weight produced the same effect.
Continue to:
My Books

