Treatment Of Diseases Of The Central Nervous System. Part 3
Description
This section is from the book "Massage Its Principles And Practice", by James B. Mennell. Also available from Amazon: Massage It's Principles and Practice.
Treatment Of Diseases Of The Central Nervous System. Part 3
Nothing need be added to what has been said as to the technique employed in treating flaccid paralysis, save to emphasise once more that no paralysed muscle should be allowed to stretch.
From the very outset every attempt must be made to secure voluntary movement, not only in the affected muscles, but also in those that have not suffered. It is in cases of poliomyelitis that the combination of muscle rest and muscle training is seen at its best. The longer the delay in starting, the more laborious is the task for patient and masseur alike. The technique has been fully dealt with. Here it suffices to add that we must beware of over-fatigue, and remember the value of "spacing" the training with massage.
Inevitably the day will come when some movement or exercise cannot be performed with a freedom equal to that of the previous day. This is a sure sign that an attempt is being made to push progress too rapidly, and the correct treatment is to maintain the muscles at rest in a position of relaxation for one or two days. Massage only should be given meantime, and the exercises should be resumed gradually.
Anyone who has had experience in the treatment of this type of case, and who has never overdone treatment, may be assured that he has not rendered full assistance to his patients; while he who has never acknowledged that he has given an excessive dose, and eased off in consequence, has assuredly inflicted great injury on some of them. In fact the test of proficiency in re-educating a case of flaccid paralysis is the ability to determine the exact moment at which rest is preferable to perseverance.
Throughout treatment all joints must be kept supple by relaxed movements, and every area of the body which is not affected should be exercised regularly and freely. During movements or exercises no paralysed muscle must ever be allowed to stretch, so that great care and ingenuity are called for in prescribing. A splint on a limb need not prevent exercise, for it is generally easy to attach a cord from the weight and pulley apparatus to a bandage which is keeping the splint in position (see Fig. 143).
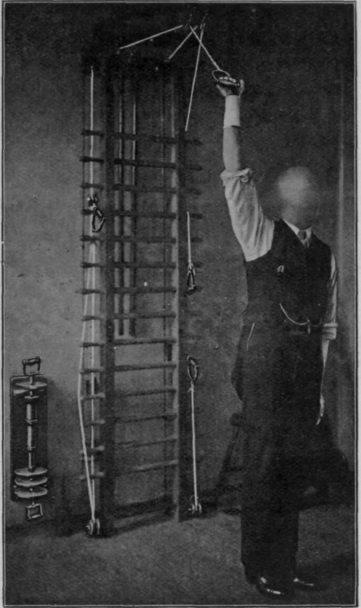
Fig. 143. - To show how a patient wearing a cock-up splint, and suffering from musculo-spiral paralysis, may safely exercise the limb with the weight and pulley. All exercises must be performed with the back to the apparatus.
All other forms of flaccid paralysis should be treated on similar lines, e.g., those due to acute myelitis or syphilitic changes. When the origin of the trouble is due to pressure by tumours or is the result of caries the outlook is very poor; but whenever gummatous change is the cause we can maintain the nutrition and mobility of the parts affected till such a time as recovery has taken place. Without this assistance the recovery of the central lesion might be in vain as regards restoration of function.
When a nerve has been severed and sutured the treatment of the paralysed muscles is similar in all detail to that prescribed for poliomyelitis. It is important to remember, however, that the fact that a nerve has been exposed by an incision renders it liable to be caught in scar tissue. Hence our duty is to apply local treatment to the scar.
For the first three weeks after operation every care should be taken to avoid performing any movement which tends to irritate the granulation tissue which holds the wound edges together. Neglect of this precaution will add to the formation of cicatricial tissue. It is usually unwise to vibrate the area until six weeks have passed. Surface stroking and gentle kneading will help much, and fine frictions may prove invaluable if there is any evidence of local "thickenings."
Reference has been made to the treatment of postural paralysis, the example selected being wrist-drop following hyper-extension of the wrist.
This trouble should be treated exactly as if a true flaccid paralysis were present. Duration of the paralysis will be short if the wrist is constantly maintained in the dorsi-flexed position; it may be very lengthy if the wrist-drop is allowed to persist. When strength is returning gentle percussion, preferably clapping, for a few moments at intervals during treatment, may prove beneficial, particularly if the disability has been only partial and transitory. Pressure paralyses will be considered in the next chapter.
Disuse atrophy may simulate a complete paralysis, and may even lead to a wasting that is apparently complete. The reaction of degeneration is usually well marked if the disuse is of long duration. It is impossible to say where the lesion exists, but certain it is that there may be a complete break in the continuity of the conduction of impulses from the centre of volition to the muscles. It may be that it is possible for a muscle, so to speak, to forget how to respond to impulses which reach it. Whatever may be the cause, treatment should follow on the lines laid down for that of the postural paralyses. During the recovery stages percussion may play a prominent part, if the atrophy is not advanced.
A victim of disseminated sclerosis is indeed to be pitied. Unless taken by some intercurrent illness, he inevitably becomes bedridden; though, fortunately, by this time the mind is usually dulled and the patient unable to resent the condition.
Actual paralysis rarely develops, as the disease is one which affects the neurogleia cells, and the axons only suffer in late stages from the pressure.
The earlier stages are often distressing, as the youthful patient battles against the onset of vague symptoms. It is typical of the disease that its progress is in waves, so that downward progress is always followed by improvement, though the patient never arrives again in statu quo ante. The aid of massage is invoked at the onset of the downward wave, and soon the upward follows. The patient gives all the credit to the massage; and it is well humbly to accept it, as it provides the patient with a sure hope of relief in future attacks.
Continue to:
My Books

