Pessaries. Part 3
Description
This section is from the book "Intra-Pelvic Technic OR Manipulative Surgery of the Pelvic Organs", by Percy H. Woodall, M. D., D.O.. Also available from Amazon: Intra-Pelvic Technic OR Manipulative Surgery of the Pelvic Organs.
Pessaries. Part 3
All of the ring pessaries have a tendency, after being worn for a short while, to shift their positions and turn edgewise to the vaginal entrance and to slip out. To prevent this a ring with a bar running crosswise its center from which a stem projects into the vagina, has been devised. This is called the Minge or Vienna pessary (Fig. 56.) The ring may be of hard rubber and the stem detachable, or the entire pessary may be made of soft rubber. The hard rubber ring is introduced as usual and the stem then secured in the opening provided for it.
The Hewitt pessary, is a tier of inflated soft rubber rings, the smallest at the upper end. It is large, heavy and fills the vagina completely. Its supporting surfaces are extensive and it has corresponding liability to irritate the vaginal walls and to collect and retain the secretions. It requires great care, frequent cleansing and prevents satisfactory douching.

Fig. 69-71. How to insert Gehrung Pessary
The Gehrung pessary, a ring first flattened and the ends of the oval then bent toward each other, is valuable in the treatment of prolapse of the uterus or of the anterior vaginal wall, cystocele. Notwithstanding its value the introduction of this pessary is somewhat difficult and complicated. First straddle the pessary over the index finger of the right hand, (Fig. 69), and then gently grasp the loop nearest you with the thumb and index finger, the palmar surface of the hand looking upward. (Fig. 70.) The hand with the pessary is turned toward the left until its dorsal surface looks upward and to your left. (Fig. 71.) The point of the loop opposite the one that is grasped (the free loop) is hooked into the vagina, the point of both loops being directed toward the patient's left, or your right. The loop held in the right hand, with a sort of screwing motion, gently pressing inward all the time, is brought downward to (Fig. 72), and then past the posterior median line and on upward toward the patient's right. (Fig. 73). As the point midway between the anterior and posterior median lines is passed, and the loop is pointing somewhat upward, it is slipped within the vagina and carried to the anterior median line. (Fig. 74.) This loop (and the pessary as a whole for that matter) has now described nearly three fourths of a circle and lies just within the vagina. It is now pushed backward until it passes the urethral opening, the opposite loop lying just anterior to the cervix, supporting the base of the bladder and perhaps the uterus also. (Fig. 75.) The pessary is supported by the natural narrowing of the vaginal outlet. I have sometimes found it necessary to spread the limbs of the anterior loop of this pessary so that it is made wider. This gives it a more secure support within the vaginal entrance.

Fig. 72-74. How to insert Gehrung Pessary (continued)
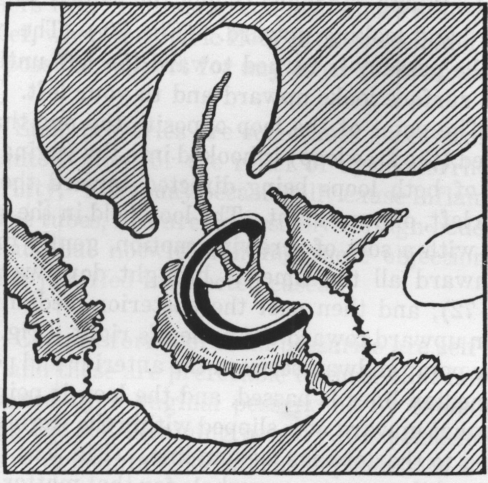
Fig. 75. Gehrung Pessary in Position.
The belt pessary is only resorted to when all others fail. It is used, and sometimes affords great relief, when the pelvic floor is destroyed and there is no possible support for any other form of pessary.
Stem pessaries are sometimes successfully used in anteflexion for the relief of dysmenorrhoea and sterility. They may occasionally cause inflammation of the tubes, and are necessarily foreign bodes in the uterus, but notwithstanding these objections their use is justified in selected cases.
Certain forms of stem pessaries are self retaining and these are preferable to those that have to be retained by a vaginal pessary or by tampons. In using the self-retaining pessary it is sometimes necessary to maintain the uterus in place with a vaginal pessary.
The intra-uterine stem is usually either grooved, or it is hollow, to allow the passage of the menstrual flow and the entrance of the spermatozoa in cases of sterility. To introduce a stem pessary it is sometimes necessary to dilate the cervix under anesthesia, though most of them are easily introduced if they are previously curved to conform to the angulation of the cervix and body of the uterus.
A stem pessary may be left in place from six weeks to two or three months if no untoward symptoms manifest themselves. The patient must be under observation during this time and if pain or marked leucorrhoea occur the pessary must be removed at once.
Pessaries require constant observation and attention.
After a pessary is fitted the patient should be required to return in two or three days to see that the uterus is retained in position and that the pessary is also in place and has not caused any degree of irritation. Of course the patient is advised to return at once should there be any inconvenience, or discomfort, or any indication that the pessary had slipped out of position.
If, after the first visit, all is well, the patient is expected to call again within a week or ten days when she is again examined. At each of these visits the pessary is removed, cleansed and replaced. Although the uterus is properly supported, the old adhesions are again stretched bimanually and the uterus is freely moved in all directions. This is repeated every two weeks until two or three months have passed when the pessary is removed.
After the removal of the pessary the patient is requested to return after two or three days, and if on examination the proper uterine position is retained, she is told to return again in ten days or two weeks. If, on examination at this time, the normal position is still maintained, the patient is asked to call again in six or eight weeks for a final examination. If all is now well, she is discharged with instructions to report again should there be any indications that the displacement has returned.
If, however, after the first visit the uterus has not maintained its position, or the pessary has slipped or has shown evidence of irritating the vaginal walls, it must be removed, reshaped and refitted or another one better adapted to the particular case, introduced. The patient must return again in three or four days to determine if this newly fitted instrument meets all indications. If it does the visits are made at longer intervals, as before indicated.
If after the pessary has been worn for two or three months and is finally removed, should there be a return of the displacement, a careful search for the cause of this should be made. There may be some remaining adhesions not sufficiently relaxed a failure of some of the factors necessary to retain the uterus in place or an improperly fitted pessary. The cause of the failure of the uterus to remain in place having been determined and remedied, if pos sible, the patient is kept under observation, as before, and the pessary again removed in two or three months. Should the displacement again recur the pessary may have to be worn indefinitely or an operation considered if the symptoms are sufficiently troublesome.
A patient when wearing a pessary, especially after it is first introduced, should take a copious douche of warm water daily. Boric acid or some other mild antiseptic may be added, if desired.
Women may wear pessaries almost indefinitely without irritation though if they are not properly fitted and cared for the irritation and inflammation caused by them may more than offset the good they may do. The toleration of the vaginal walls is almost incredible in some instances. I once removed a hard rubber ring pessary that had been in place without removal for at least thirty years. A patient of nearly seventy complained of a leucorrhoea and upon examination the pessary was found. It was considerably eroded where it fitted in the posterior vaginal fornix and at which point it was almost embedded in the tissues. It was removed without difficulty and with the use of mild antiseptic and cleansing douches the leucorrhoea ceased in a few days.
Continue to:
My Books

