2. Chronic Interstitial Hepatitis. Cirrhosis
Description
This section is from the book "A Manual Of Pathology", by Joseph Coats, Lewis K. Sutherland. Also available from Amazon: A Manual Of Pathology.
2. Chronic Interstitial Hepatitis. Cirrhosis
We have to do here with a chronic inflammation of the interstitial connective tissue of the organ.
Causation
As the disease occurs for the most part homogeneously throughout the organ, the irritant is contained in the blood circulating in the liver. The name "gin-drinker's liver," frequently applied to this disease, involves the view that alcohol is commonly the irritant. Alcohol taken frequently in the form of undiluted spirits is believed to cause the disease, while beer and wine do not. But the disease may originate from other kinds of irritation whose nature is obscure. It has been produced experimentally by chronic poisoning with phosphorus and cantharides, and it probably occurs also as a result of syphilis. It has been met with in young children, and the author has recorded a case in which a typical cirrhosis, with the usual secondary phenomena, occurred in a cat. The fact that it was a butcher's cat may indicate that it indulged in excess of eating rather than of drinking. Greenfield has also recorded two cases of cirrhosis in the cat.
It has been asserted of recent years that obstruction of the bile ducts is a cause of cirrhosis, and a special form of Biliary cirrhosis has been distinguished. There are undoubtedly cases which have this origin, but, on the other hand, there are many cases of biliary obstruction with no such result. In any case biliary cirrhosis forms a small proportion of the cases of cirrhosis, and on the whole the disease is hematogenous in its origin..
Character Of The Lesions
In cirrhosis we have chronic inflammation of the connective tissue of the liver, resulting in new-formation of a similar tissue. The interstitial connective tissue of the liver follows, as we have seen, the portal vessels, forming a frame-work in which are supported the portal vein and its branches, the hepatic artery and hepatic duct. The new-formation occurs in the great majority of cases only in these regions, that is to say, outside the lobules. In the earlier stages the affected connective tissue is abundantly cellular, like granulation tissue, and the process of new-formation is evidently similar in its details to that in other chronic inflammations (see Fig. 408).
As a general rule the new-formed tissue undergoes development into dense connective tissue which has a tendency to shrink. By its shrinking it causes Atrophy of the proper hepatic tissue. As the cirrhosis is usually multilobular the contracting tissue isolates groups of lobules of larger or smaller size, and these, consisting of soft tissue, stand out somewhat when the liver is divided, or present themselves prominently at the surface. There are thus areas of remaining hepatic tissue which are being gradually encroached on by the connective tissue. The atrophy of the hepatic tissue takes place by the supply of blood being cut off. By the contraction of the new-formed tissue the portal vessels, and especially the interlobular branches, are narrowed. The hepatic artery is not much affected by the contracting tissue. Indeed, as the hepatic artery supplies the active connective tissue there is a new-formation of capillary blood-vessels in connection with its terminal branches. Injected preparations show that the hepatic artery is pervious, and that the new-formed connective tissue is highly vascular.
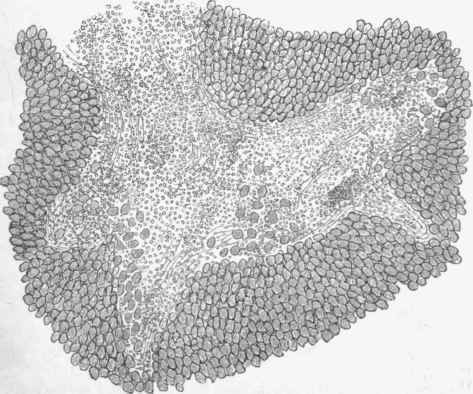
Fig. 408. - Cirrhosis of liver in early stage. The connective tissue is occupied by numerous round cells which are involving the peripheral parts of the lobules, the hepatic cells being here frequently isolated in the midst of the round cells, x 75.
The destruction of the hepatic cells takes place to a large extent by fatty degeneration, and one can often see, in the midst of connective tissue, islands representing hepatic tissue consisting of little more than collections of oil drops (see Fig. 409). The hepatic tissue is also commonly stained with bile pigment of a yellow or brown colour, and this we may associate with obstruction of the bile ducts by the contracting connective tissue. For the most part the pigment is biliary, but it is also to some extent blood pigment arising from the obstruction to the circulation. The connective tissue is also commonly stained, and to the naked eye the cut surface has a yellow colour, sometimes with here and there quite an orange tint. The name of the disease, cirrhosis, was originally applied from the colour of the altered organ.

Fig. 409. - Cirrhosis of liver in an advanced stage, shown with a very low power. There are great areas of fibrous connective tissue, in the midst of which are islands of hepatic tissue having an opaque appearance from the presence of fat in the cells, x 20.
A prominent feature in microscopic examination in many cases is the presence of narrow elongated canals, lined with epithelium, which are usually described as Capillary bile ducts. They are present in the midst of the connective tissue, sometimes very abundantly, and, as no such ducts exist there normally, they are in a certain sense new-formed.
By some authors (especially Charcot and Gombault) they are regarded as entirely new-formed, and their existence is taken as characteristic of a special form of cirrhosis. They are, however, to be found in all forms of cirrhosis, and they are probably to be regarded as the biliary capillaries, which have survived the destruction of the hepatic tissue. The larger bile ducts, which run in the capsule of Glisson, are unaltered, not being apparently affected by the shrinking connective tissue.
In its macroscopic appearances the liver varies considerably. In the earlier stages it is enlarged, but as a result of the changes detailed above it undergoes atrophy and distortion. The connective tissue contracts, and as it is irregularly distributed the contraction is irregular. The surface of the organ presents larger or smaller projections consisting of the less affected hepatic tissue between the cicatricial depressions. These projections may be comparatively large, forming the Hob-nail appearance of the surface, or they may be smaller, giving a generally granular appearance. They are usually yellow or brown and opaque, being fatty and stained with pigment. Sometimes there is special shrinking of the left lobe, and generally there is dragging in of the edges, so that the liver assumes more of a compacted form, being perhaps even thicker than usual, but reduced in superficies. It is dense to the feeling, and more tough to cut than normal. On the cut surface it may be possible with the naked eye to make out the grey connective tissue, with islands of opaque or pigmented hepatic tissue in it.
The terms Biliary cirrhosis and Hypertrophic cirrhosis are in frequent use, especially in French medical literature. The former of these was used by Charcot to indicate the mode of origin of the affection, the expression indicating that the irritation extended from the bile-ducts. This form was distinguished in its causation from the haematogenous or venous, in which the irritation extended from the blood-vessels. The biliary form arises in connection with obstruction and inflammation of the bile ducts. In this form there are, according to Charcot and Gombault, two distinctive features, namely, (1) that the new-formation of connective tissue exists somewhat uniformly, so that the individual lobules are surrounded by it - the so-called Monolobular cirrhosis; and (2) that the capillary ducts already referred to are visible. To this last condition great importance has been attached.
It is to be acknowledged as a result of experiment that obstruction of the bile ducts leads to an increase of connective tissue in the liver, and to a monolobular cirrhosis. In man such a result sometimes follows on biliary obstruction. It did so in a case observed by the author of congenital stenosis of the bile ducts. There was great biliary infiltration and an extreme monolobular cirrhosis. At the same time, as cirrhosis is by no means a constant result of biliary obstruction, there must be an element yet to be elucidated.
Hypertrophic cirrhosis is a name given by another French author, Hanot, and it applies to the same" class of cases. The biliary monolobular cirrhosis is characterized by hypertrophy of the liver.
The ordinary alcoholic cirrhosis in its early stage may show considerable hypertrophy, the new-formation may be monolobular in its distribution, and there may be the most marked new-formation of capillary ducts.
The author is able to refer to a case which he examined post mortem. It was carefully watched for six weeks during life by Sir William Gairdner. When first observed there was great enlargement of the liver, and there was reason to believe that it had been greater. The patient had been addicted to alcohol for over two years. There were haemorrhages from stomach and bowels, and marked ascites, but little or no jaundice. After death the liver was found small, weighing 43 oz., and finely granular on the surface. There was a great excess of connective tissue, which presented many round and spindle-shaped cells, and was monolobular in its distribution. The hepatic cells contained abundant fat in small and large drops. In this case the cirrhosis, although monolobular and at one period hypertrophic, was not connected with obstruction of the bile ducts.
Outside the liver the principal changes depend on Obstruction of the portal circulation. The connective tissue narrows the portal vessels in the liver, and this leads to a chronic passive hyperemia in all the radicles of this vein, in the peritoneum, in the mucous membrane of the stomach and intestine, in the spleen, and so on. The most frequent consequence is ascites, but we also meet with haemorrhages from the mucous membranes, especially of the stomach and large intestine, as well as catarrh. The spleen also is enlarged. Occasionally thrombosis of the hepatic vein results, and this may extend to the vena cava. A very large haemorrhagic infarction of the lung was observed by the author as a result of embolism from a softened thrombus of this kind.
The obstruction of the portal vein often leads to widening of the venous channels which form communications between the portal radicles and the Systemic veins. In this way we may have great dilatation of the internal hemorrhoidal veins (leading to piles) and of the hypogastric. The cutaneous branches of the latter often stand out prominently on the abdominal wall. The hemorrhoidal veins also communicate with the vesical, and these latter may undergo dilatation. There may also be widening of communications with the veins of the diaphragm and oesophagus, which have sometimes been found highly varicose. Another channel occasionally met with is a small vein which runs from the portal vein to the umbilicus. In some cases this is so much enlarged as to approach the size of the portal vein itself.
The patient generally dies from the disorders due to the continuous passive hyperemia - the persistent catarrh of the alimentary canal, perhaps with haemorrhages, the ascites, etc. There is great emaciation and sometimes icterus. It is not clear that the mere loss of the function of the liver bears an important part in the fatal result.
Continue to:
My Books

