4. Atheroma. Chronic Endarteritis. (Arteriosclerosis, Endarteritis Deformans, Endarteritis Nodosa)
Description
This section is from the book "A Manual Of Pathology", by Joseph Coats, Lewis K. Sutherland. Also available from Amazon: A Manual Of Pathology.
4. Atheroma. Chronic Endarteritis. (Arteriosclerosis, Endarteritis Deformans, Endarteritis Nodosa)
These names are applied to a disease of very frequent occurrence in arteries, the nature of which has been differently regarded at different times.
(A) Causation And Nature Of The Disease
According to the more common view of the process the disease is an inflammation- of the internal coat, and hence the name endarteritis. But there are several indications which tend to remove atheroma from the category of a simple endarteritis. The thickening of the intima, which is the primary feature, partakes of the nature of a hypertrophy, the- new tissue being more special in structure than the ordinary new-formed tissue of inflammation (see below). It is also a tissue which tends to degeneration, mostly fatty degeneration. The fact that the disease is peculiarly one of advanced life is another fact of importance, and it may also be said that a weakness of the wall of the vessel must be regarded as one of the principal agents in the causation of the disease. While there is this predisposition the actual supervention of the disease is apparently caused by mechanical irritation. Its principal seat is the arch of the aorta, and this is doubtless due to the fact that this part is more exposed to the force of the wave of blood during the systole of the heart than any other portion of the arterial system. The disease is frequently met with in the arteries of the brain, and here it is more difficult to account for its occurrence on the theory of mechanical irritation, but the atheromatous patch is often situated just at a bifurcation, where, presumably, the vessel wall is more exposed to the force of the current. It is also common, as already remarked, in the coronary arteries, where we may presume that the blood pressure is higher than in other arteries of their size. Again, it is met with in the pulmonary artery in cases of hypertrophy of the right ventricle, the excessive impulse of the blood from the hypertrophied ventricle apparently determining its occurrence. As we shall see afterwards, syphilis produces a disease of arteries in some respects similar to atheroma.
(B) The Tissue Changes
The disease consists in a more or less localized thickening of the internal coat. The thickening is nearly always distinctly limited in area, so that we speak of Atheromatous patches (hence the name endarteritis nodosa). When we examine the aorta in the earlier stages we see elevated areas with tolerably abrupt edges, and usually of a dead white colour as compared with the surrounding intima. These patches are hard, and cut like cartilage. In the arteries of the brain the diseased parts are seen, without opening the vessels, as white opaque patches, and the vessel is more rigid than normal, so that it does not collapse; the calibre also is diminished, sometimes very greatly, by the inward projection of the patch. On cutting into the patch, in either the aorta or a cerebral artery, there is often an opaque yellow colour revealed in the deeper parts, and this is an indication of fatty degeneration. Very often, too, there is, especially in the aorta, calcareous infiltration of the deeper parts of the patch, but these two conditions will be more fully discussed further on.

Fig. 236. - Beginnings of atheroma in a small artery. There is thickening of the intima, with abundant cell-formation. The membrane of Henle is seen as a sinuous band, x 370.
In considering more particularly the details of the process, it is instructive to examine microscopic sections, including the edge of the patch and the neighbouring parts of the vessel. In well-preserved recent cases it can be seen that the endothelium of the intima is continued over the patch, a cellular proliferation in the sub-endothelial tissue is seen to be the essential feature (Fig. 236). In nearly all cases there is little difficulty in observing that the patch is really a thickening of the internal coat, as shown in Figures 237 and 238. The thickened intima is composed of a dense connective tissue, which in the early stages contains many round, oval, and stellate cells. In many cases the thickened intima can be made out to present a similar structure to the normal intima. A section on the flat shows large numbers of branching cells (as in Fig. 239), such as characterize the normal structure. The new-formed tissue thus constitutes a hypertrophy of the intima.

Fig. 237. - Edge of patch in atheroma of femoral. To the right the membrane of Henle is seen as a dark band. The patch has broken through the membrane and projected itself into the middle coat, x 40.
In a fully formed patch the structure is often somewhat indefinite. The tissue is indeed half obsolete, and, as already indicated, fatty degeneration readily occurs. The fatty degeneration begins usually in the deeper layers of the patch, so that on cutting into it one generally finds in the portion of the patch bordering on the middle coat an opaque yellow streak (see also Fig. 240). The fatty degeneration at first affects the cells of the intima (as shown in Fig. 240), but as time goes on the intercellular substance gives way, and the tissue breaks down, so that a cavity containing fatty debris with crystals of margarine and of cholestearine is formed. It is from the character of this fatty debris that the name atheroma is derived, and the cavity thus formed is sometimes called an Atheromatous abscess. (See Fig. 241).
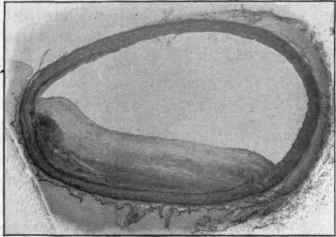
Fig. 238. - Atheroma of femoral artery. The disease consists in a localized thickening of the intima forming the atheromatous patch, x 6.
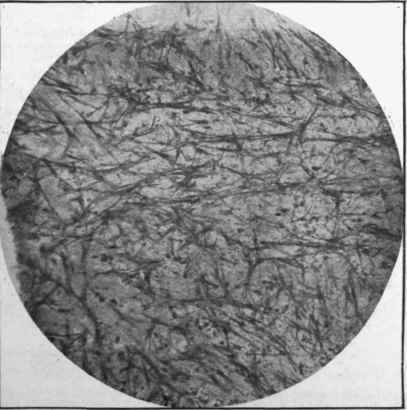
Fig. 239. - Section of atheromatous patch on the flat. It is seen to present stellate cells with elongated processes, x 350.

Fig. 240. - Atheroma of aorta. The internal coat(a) is seen to be thickened. In its deeper layers there are darker markings indicating the commencement of fatty degeneration; 6, middle, and c, external coat, x 22.

Fig. 241. - Atheroma of femoral artery. The greatly thickened internal coat (a) is shown: In the midst of it, towards the right, are dark masses consisting mainly of fatty debris, and representing the atheromatous abscess. At one part the middle coat (6) is considerably encroached on from within, x 22.
The tissue superficial to the cavity may ultimately give way, and so expose the cavity, thus forming an Atheromatous ulcer. (See Fig. 242.) The ulcer sometimes presents calcareous masses in its walls, and in any case it may induce the deposition of fibrine on its surface.
Continue to:
My Books

