Anatomical Changes In Phthisis. Part 3
Description
This section is from the book "A Manual Of Pathology", by Joseph Coats, Lewis K. Sutherland. Also available from Amazon: A Manual Of Pathology.
Anatomical Changes In Phthisis. Part 3
(B) The Fibroid Form
On post-mortem examination in typical cases of this form the lung is found very firmly adherent over the affected part, which nearly always includes the apex. One often has to remove with difficulty a dense leathery cap which covers the apex of the lung (see Fig. 369). On cutting into the lung there are usually cavities, but they are not generally large and the internal surface is mostly clean and moderately smooth. A distinct membrane lines the cavity (c in figure). Outside the cavity the tissue is of a deep slaty colour in which opaque white spots may be occasionally visible, and it is very dense. The dense pigmented tissue may involve a considerable portion of the lung and the affected part is shrunken and contracted (see figure).

Fig. 369. - Upper lobe of lung in fibroid phthisis, a, a, greatly thickened pleura; b, condensed and pigmented tissue; c, cavity with distinct lining; d, bronchial glands enlarged and pigmented; e, main bronchus. The nearness of the bronchus and glands to the apex indicates the shrinking. Nearly natural size.
Looking away from the condensed part in which the lesion is advanced, we find, as in the caseous form, the advanced posts of the disease in the form of isolated condensations in the midst of the crepitating normal tissue. Here the Initial lesion is different from that in the other form. It consists in hard dark or nearly black solid bodies, scattered through the lung tissue. On running the finger over the cut surface one feels these bodies and they stand out above the general surface.
In this form as in the other a plugged bronchus will be found to form the centre of the initial lesion. This is shown in Fig. 370, which is from the centre of such a lesion. The bronchus contains, as before, inflammatory products, namely, round cells and desquamated epithelium. The wall of the bronchus is also infiltrated with round cells, and tubercles are present in the wall and in the surrounding connective tissue. There is, however, Very little appearance of inflammation in the lung alveoli, and the affection seems to advance rather by the lymphatics into the connective tissue than along the mucous surface to the alveoli.
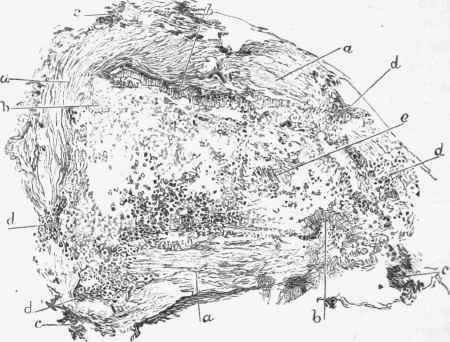
Fig. 370. - Fibroid phthisis, early lesion, a, a, bronchial wall; b, b, projecting parts still covered -with epithelium; d, d, round cells infiltrating bronchus; e, exudai tion in calibre, x 60.
The distribution of the Tubercles is indicative of the advance in the directions just mentioned. They are often grouped in the neigbour-hood of bronchi, as in Fig. 371, but are also present at some distance (a to left in figure), the process travelling by the lymphatics. The tubercles present in the earlier periods the typical structure, and there are frequently giant-cells in their midst.
Haemorrhage is very common here as in the other form, and it may be sufficient to fill out the alveoli.
Caseous necrosis is much less a feature here than in the other form, but it is usually present in the plug which fills the bronchus, as well as to some extent in the bronchial wall. This is shown in Fig. 372, in which the central part (a) representing the plug is homogeneously granular, while the walls of the tube are infiltrated with round cells. In some places (as at c) there is an aggregation which with a higher power is seen to be a tubercle.

Fig. 371. - Fibroid phthisis, a, a, tubercles in connective tissue, some close to a bronchus, others removed; the darker centres indicate caseation, e; 6, 6, emphysematous lung tissue, x 20.
A feature present in this form, but not in the other, is Fibroid transformation, which affects both tubercles and connective tissue and gives its peculiar characters to this form of phthisis. The tubercles are converted into clear structureless bodies in which all the elements of the tissues are lost except, occasionally, one or two giant-cells. These may be partly transformed, but may still be recognizable, especially as they frequently contain a considerable number of black granules.
A similar fibroid transformation affects the connective tissue around the bronchus and extends to the general stroma of the lung. There is thus great induration of the lung tissue and the fibrous tissue shrinks and produces great deformity. The shrinking of the tissue, associated as it is with adhesion of the pleura, frequently leads to drawing in of the chest wall, which is often a characteristic feature, and it leads also to two lesions which are often very apparent in the lung, namely, bronchiectasis and emphysema, both of which are complementary.
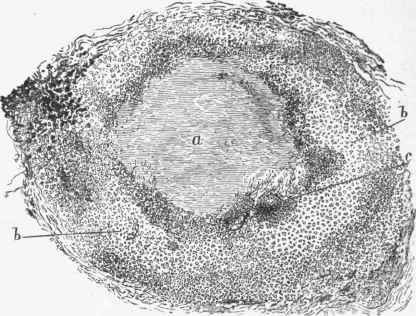
Fig. 372. - Fibroid phthisis, a, bronchus plugged and caseous; b, b, wall of bronchus infiltrated with round cells and tubercles; c, tubercle in wall.
Bronchiectasis is, in this form, the most active factor in the formation of cavities. It is partly a purely complementary process the shrinking being compensated by the dilatation of the air-spaces. Hamilton and others have pointed out another mode of formation. As the chest wall forms a comparatively fixed point to which the shrinking tissue is attached by the pleural adhesions, and as this tissue is also attached to the walls of the bronchi, the result of the shrinking will be that these two points will be approximated, the chest wall drawn in and the bronchial wall drawn out. There is a third way in which bronchiectasis occurs. The secretions may accumulate in a bronchus behind an occlusion of the tube. Such an occlusion will occur when the primary lesion has affected a bronchus of larger calibre than usual, or where the shrinking tissue has constricted a bronchus.
Continue to:
My Books

