Diseases Of The Pericardium
Description
This section is from the book "A Manual Of Pathology", by Guthrie McConnell. Also available from Amazon: A Manual Of Pathology.
Diseases Of The Pericardium
May have hydro pericardium, a collection of non-inflammatory transudate within the sac. This is usually a part of a general dropsy due to disease of the heart, kidney or liver. Hemopericardium, when containing blood which gains entrance from rupture of the heart, of aneurysms of the great vessels or wounds. If in large amount it causes death by mechanically interfering with the contraction of the heart.
Pericarditis is seldom primary, but is usually secondary to infectious diseases, such as acute rheumatism, scarlet fever, pneumonia, endocarditis and pyemia. It may result from the extension of inflammation from neighboring tissues.
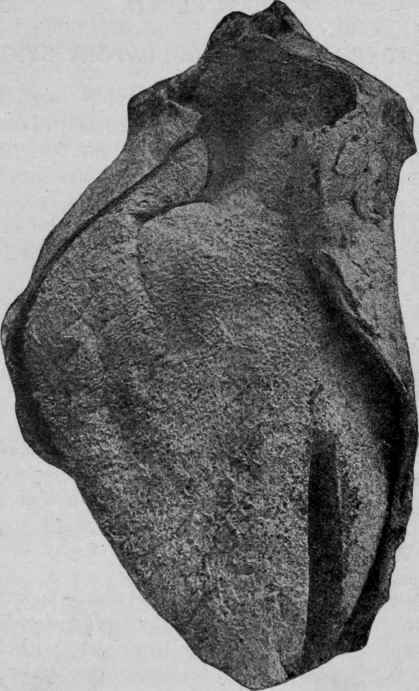
Fig. 131. - Acute Pericarditis (Bramwell).
The inflammation may vary greatly, and according to the exudate various forms of pericarditis are described such as fibrinous, serofibrinous, and purulent. There is at first a dulness of the serous membrane as a result of changes in the endothelium and the formation of a delicate layer of fibrin, and later a serofibrinous exudate. This may be slight or there may be 1000 to 2000 c.c. of fluid. The pericardium may become thickened, roughened, and covered by a coating of fibrin that may be quite marked. At the apex the fibrin is collected into strands, giving a villous appearance to the heart, the cor villosum. At the base of the heart, where the movements are more restricted, there is a "bread and butter" appearance.
As the serum is absorbed the fibrin may be replaced by connective-tissue adhesions until the pericardial sac is either partially or completely obliterated, adhesive pericarditis. As a result of this, marked hypertrophy may ensue and also some degeneration of the myocardium. Occasionally there is a deposit of lime salts in the organized tissue.
In the early stage there is microscopically a degeneration of the endothelium, which is covered by a layer of fibrin, and a round-cell infiltration of the subendothelial tissue.
Purulent Pericarditis
Purulent Pericarditis generally results from the extension of suppuration of some neighboring organ. The most common organisms found are the streptococci, diplococci pneumoniae, staphylococci and the tubercle bacilli. It may start as a simple inflammation and later on give rise to a purulent exudate. The pericardial sac contains more or less purulent or seropurulent fluid. The myocardium is usually involved superficially; it becomes edematous, infiltrated with pus, and may undergo fatty degeneration; at times inflammation, myocarditis, may occur.
Tuberculous Pericarditis
Tuberculous Pericarditis is commonly a part of a general miliary infection, or it may result from an extension from a neighboring lesion of the pleura. The exudate is frequently blood-stained. Both the visceral and parietal layers of the pericardium may show considerable thickening. The lesions found are similar to those occurring in tuberculosis in other parts.
Milk spots are irregular whitish areas found on the external surface of the heart. They probably result from constant pressure and are more accurately known as friction scleroses.
Some may be the results of a previous inflammation. There is a thickening of connective tissue below the endothelium.
Tumors
Sarcoma and carcinoma occur as secondary growths either from infiltration or as metastatic tumors.
Myocarditis or inflammation of the heart muscle is usually secondary to infectious conditions elsewhere, particularly in pericarditis. May be acute or chronic, diffuse or circumscribed.

Fig. 132. - Chronic Interstitial Myocarditis. (Fibrous replacement hyperplasia.) [Delafield and Prudden].
In the acute circumscribed form numerous small metastatic abscesses are present. Beginning as minute infectious emboli in small vessels, generally in cases of malignant endocarditis, degeneration and necrosis may ensue, so that an abscess cavity the size of a cherry may develop. The contents are composed of pus, broken-down muscle and bacteria. This may perforate into the cavities of the heart, into the pericardium, or may form a cardiac aneurysm. The abscess may lose its liquid contents, become encapsulated or infiltrated with lime salts.
In the acute diffuse variety, as seen in diphtheria and scarlet fever, there is a diffuse round-cell infiltration between the muscle fibers with proliferation of the connective-tissue cells as well. The muscle fibers become granular, opaque, and the striations indistinct: They may undergo Zenker's hyaline degeneration. If the patient recovers scar tissue may form. This condition occurs in scarlet fever, diphtheria, typhoid, gonorrhea, etc.
The heart is soft and friable, and usually lighter in color than is normal, and the fibers are easily separated. Dilatation of the left ventricle is often present.
In chronic fibrous myocarditis the lesions may be diffuse or localized. It may be the result of a former acute diffuse myocarditis or it may be secondary to diseases of the coronary arteries or to disturbances of their circulation. This leads to degeneration or necrosis of the muscle and a new formation of fibrous tissue, a replacement hyperplasia, probably not inflammatory. In the muscle are seen spots or streaks of sclerotic tissue. Microscopically greater or less amounts of connective tissue are found separating the fibers which frequently undergo a fatty degeneration as a result of pressure and thus give rise to irregular yellowish areas.
Some of the sclerotic portions found along branches of the coronary artery probably represent healed infarcts.
Continue to:
My Books

