Diseases of Pancreas
Description
This section is from the book "A Manual Of Pathology", by Guthrie McConnell. Also available from Amazon: A Manual Of Pathology.
Diseases of Pancreas
Malformations are unusual, except that the pancreas may frequently be composed of separated segments. Fragments of pancreatic tissue are sometimes found in the omentum, the walls of the intestine or of the stomach. Variations of the ducts are very common. The duct of Wirsung may be double, its relation to the duct of Santorini may vary greatly. Both ducts may open separately into the duodenum. Usually the duct of Wirsung and the common bile-duct open into the diverticulum of Vater.
Active hyperemia is present during digestion and as a stage in inflammation. Passive hyperemia occurs when there is some obstruction to the portal circulation. Is common in alcoholics and may lead to the formation of connective tissue.
Acute hemorrhagic pancreatitis is an uncommon condition of unsettled origin. It occurs in men rather than in women and seems to be associated in many cases with cholelithiasis. By obstruction of the diverticulum of Vater bile may be forced up into the duct of the pancreas and give rise to hemorrhagic pancreatitis. Various irritating substances when injected into the duct of Wirsung have given rise to a similar condition. The greater part of the pancreas is generally involved and death frequently comes on quite suddenly. Microscopically there is found extensive necrosis of the parenchyma and of the interstitial tissue as well. The stroma is the seat of a marked round-cell infiltration and the fat frequently contains areas of necrosis. The epithelium is the seat of fatty degeneration and may be no longer recognizable.

Fig. 162. - Chronic Interstitial Pancreatitis Following Duct Obstruction, showing Islands of Langerhans unchanged though Embedded in Sclerotic Tissue (Opie).
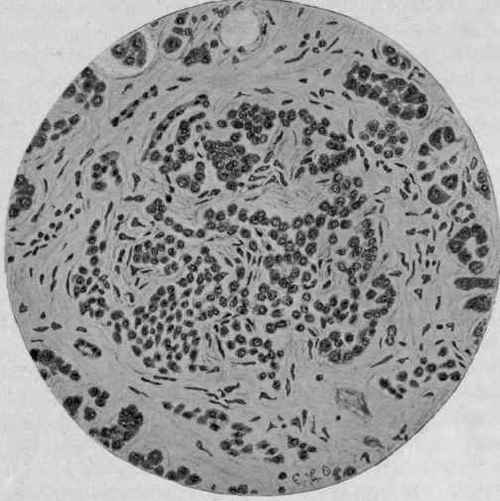
Fig. 163. - Chronic Interstitial Pancreatitis of Intra-acinar Type, showing the Invasion of an Island of Langerhans by the Inflammatory Process (Opie).
Blood-vessels may be eroded and hemorrhage occur. Is impossible to sharply separate pancreatic hemorrhage from hemorrhagic pancreatitis.
Purulent pancreatitis may originate as such primarily or it may follow the hemorrhagic form. There may be a diffuse leukocytic infiltration or a formation of miliary foci of suppuration with here and there distinct abscesses. The infection may be due to the extension of inflammatory processes of a neighboring organ.
Gangrenous Pancreatitis
Gangrenous Pancreatitis in many cases is a sequel of the acute hemorrhagic or it may follow the purulent variety. The gland is swollen, dark red, and soft; and may be converted into a dark, slate-colored, bad smelling mass. The entire gland may at last be changed into a large necrotic mass. Accompanying these changes numerous scattered foci of fat necrosis occur.
Chronic Or Interstitial Pancreatitis
Chronic Or Interstitial Pancreatitis is characterized by an overgrowth of fibrous tissue with more or less atrophy of the parenchyma. The connective tissue may be increased, either interlobular or intra-acinar. In the interlobular variety the islands of Langerhans are unchanged, while in the intra-acinar form the fibrous tissue surrounds and invades them. It is at times associated with cirrhosis of the liver.
Syphilitic Pancreatitis
Syphilitic Pancreatitis is not unusual in congenital cases. There is diffuse proliferation of fibrous tissue between the lobules and the acini. The cells also atrophy and disappear and the blood-vessels are the seat of a periarteritis. The islands of Langerhans are not affected. Gumma is rare, a few cases only having been reported.
Tuberculosis
Tuberculosis is infrequently met with, but may occur in the miliary form or, what is more rare, as a large caseous mass.
Atrophy of the pancreas is frequently found in old age, in local disturbances of the circulation, cachexia, diabetes, and emaciation.
Hanseman's Form Of Atrophy
Hanseman's Form Of Atrophy is consequent upon chronic inflammation. The organ is diminished in size and flattened, the fibrous tissue is usually adherent to adjacent organs, the epithelial elements are atrophic and are in part replaced by connective tissue. Hanseman thought that this form of atrophy was always present in cases of diabetes. Opie has found, however, that it is only in the intra-acinar form in which there is a hyaline degeneration of the islands of Langerhans that diabetes occurs.
Fatty infiltration is not infrequently found accompanying various of the infectious fevers. The fat is deposited chiefly in the interlobular connective tissue and causes a secondary atrophy of the parenchymatous cells which may also contain some fat. The organ may be a trifle enlarged, soft, and grayish in color.
Fatty metamorphosis occurs as a result of severe infection, as in chronic phosphorous poisoning. The organ is soft and cloudy white.
Fat Necrosis
Fat Necrosis is a peculiar form of degeneration taking place in the fatty tissues of the pancreas and omentum. It appears as small, opaque, sharply circumscribed, white areas in the immediate neighborhood of the pancreas or scattered throughout the organ itself. Several areas may become confluent and involve a large portion of the pancreas. The necrotic areas may be more widely disseminated, involving the omentum and the subperitoneal and the retroperitoneal tissue. They are opaque, whitish or yellowish, are sharply defined from the normal fat, and are generally surrounded by a narrow hemorrhagic zone. Their size varies from a pin's head to that of a pea, sometimes larger.
Microscopically the affected tissues show absence of nuclei with presence of fat crystals and lime salts.
This form of necrosis is due to obstruction of the outflow of the secretion, or to the escape of the pancreatic juice into the peritoneal cavity. A fat-splitting ferment is present and it breaks up the fat into glycerin and a fatty acid. The acids are deposited as needle-like crystals with the broken-down cell. The glycerin is absorbed and the acids unite with calcium to form calcium salts, which give a gritty feel when the tissue is cut.
In the majority of cases fat necrosis is associated with either hemorrhagic or gangrenous pancreatitis.
Amyloid degeneration is found in cases of general amyloid disease, occurring either in spots or in streaks.
Hyaline degeneration is met with quite frequently. It involves the islands of Langerhans as well as the parenchymatous tissue. The affected portions stain with eosin and picric acid, but do not give the amyloid reaction.
This lesion is thought to have a distinct relation to diabetes mellitus. The islands of Langerhans are most numerous in the tail of the pancreas. In certain cases of diabetes there has been a marked absence of these bodies, due to hyaline change. The parenchymatous cells in such cases may or may not be involved. It would appear that as long as the islands remain unaffected diabetes will not be present, no matter how seriously involved the parenchyma is. These peculiar bodies of Langerhans apparently exert a distinct influence upon the metabolism of sugar.
As diabetes can be caused by lesions of the fourth ventricle it is evident that all cases cannot depend upon pancreatic lesions, but there is a distinct association in many cases.
Pigmentation may be due to hemorrhage, to atrophy, or old age. The epithelial cells contain brownish or yellowish granules that do not give an iron reaction.
Hemochromatosis is a form of chronic intra-acinar pancreatitis plus the deposit of an iron-containing pigment in the liver, pancreas, other glands, and the skin. Is accompanied by a degeneration of the parenchymatous cells and a chronic interstitial inflammation of the organs. May be present in bronzed diabetes.
Tumors
Sarcoma is rare, but the round-cell and angiomatous forms have been described. They may occur as a part of a secondary sarcomatosis.
Carcinoma may occur primarily or after a similar growth in the stomach, duodenum, or gall-bladder. The primary form is found in the head of the gland and is most commonly scirrhus. It soon spreads and forms a large mass involving the greater part of the pancreas and the adjacent tissues. As it grows it may obstruct the bile-ducts, giving rise to an icterus that gradually increases in severity, or by pressure upon the duct of Wirsung set up a chronic interstitial pancreatitis'sometimes accompanied by diabetes.
The growths generally originate from the cells of the acini and give an adenomatous structure to the tissue. They may arise from the cylindric epithelium of the ducts and form a scirrhous mass, Obstruction of the pancreatic duct may cause it to become greatly dilated, so much so as to cause actual cyst formation. The contents are usually clear, but by infection may become purulent. Occasionally small cysts may be scattered through the organ.
Calculi in the duct are sometimes found. They may be a cause of obstruction.
Cysts occasionally occur. May be due to a retention of the secretion on account of obstruction of the ducts; such are usually small. Multilocular papillary cysts may result from a proliferation of the epithelial elements. Hemorrhagic cysts may follow severe traumatism.
The cystic contents are generally viscid, but may be clear and watery, or else contain varying amounts of blood. Ferments may be present.
Continue to:
My Books

