Abscesses. Part 3

Description
This section is from the book "Diseases Of The Rectum And Pelvic Colon", by Martin L. Bodkin. Also available from Amazon: Diseases of the rectum and pelvic colon.
Abscesses. Part 3
The Pelvis-rectal Abscess has its origin in the loose connective tissue existing between the elevators an and the peritoneum above, in what is known as the superior pelvis-rectal space.
Retro-rectal Abscess. This variety of abscess forms in the space between the sacrum and the rectum, in the superior pelvis-rectal space, posterior
The connective tissue of the pelvis-rectal space is part of the common connective tissue of the mes-rectum in the male and female-of the broad ligaments in the female and of that covering the prostate gland and neck of the bladder in the male.
Infection may have been carried through the lymphatics or the blood supply from adjacent pelvic disease, rectal operations, or sepsis during the puerperal The pus is liable to pass downward, penetrating the fibers of the elevators an at the junction of the elevators an and external sphincter, posterior, forming an mischief-rectal abscess also. These abscesses are always serious, the prognosis is variable and dependent on the true seat of origin. A diffuse cellulite is extremely dangerous to life as peritonitis is most easily induced should the pus burrow into the general peritoneal cavity. A deep anterior horseshoe fistula, recto-urethral fistula, or the posterior horseshoe fistula may result. The posterior horseshoe fistula follows the pelvis-rectal abscess much more frequently, however. Symptoms. The symptoms are masked by the complicating disease and appear suddenly. The invasion may be acute or extending over a period of time largely associated with the existing disease.
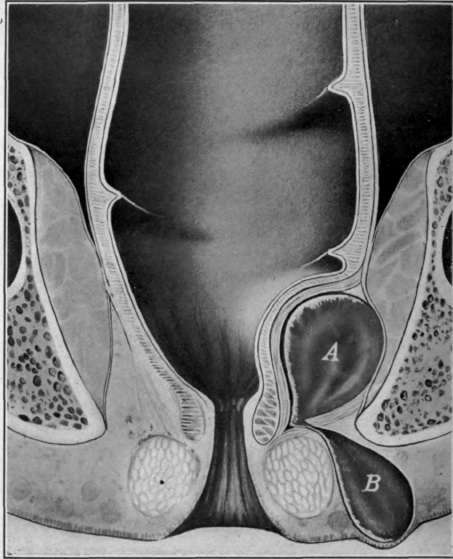
Fig. 52. Rectal abscesses. A, pelvis-rectal abscess; B, terminating in correctional abscess
Treatment
When the abscess points into the mischief-rectal Fosse the treatment is the same as for one originating in that region. Free exit for the pus will greatly ameliorate the symptoms due to the disease itself. The further treatment is mostly directed to the origin of infection and may require the vaginal incision of a pelvic abscess or, in a very exceptional number of cases, abdominal section. When this incision is carried high up through the elevator an muscle, the wound should be tightly packed for a few days to avoid hemorrhage. The incision should not be carried through the internal sphincter, otherwise incontinence will follow.
The After-treatment of incised abscess cavities is sometimes most important, as the incision may be the most radical and best method of treatment for the immediate relief from pain and suffering in general, but will not insure the patient from the discomfort and misery of a protracted fistula discharging itself from the former site of infection in the pelvic or mischief-rectal region. Therefore more failures or resultant fistulous tracts may be attributed to the lack of knowledge on the part of the surgeon, or to his inability to impress upon the patient the great necessity of after-treatment. To avoid such a result persistent treatments should be carried on at short intervals - every other day - until the fistulous tract is entirely healed. Ordinarily a pelvic-rectal or deep correctional abscess will require eight to ten weeks of treatment to bring about a successful termination. Nitrate of silver in from 5 to 20 per cent. solution will be found most useful in the healing of these tracts, after thorough irrigation of the wound with a 5 to 10 per cent. solution of tincture of iodine. To stimulate granulation ichthyology or balsam of Peru is preferred by some surgeons, but the nitrate of silver will be found the safest to guard against a tubercular invasion in those cases which manifest the disease locally in the form of one of these abscesses.
Often we are negligent in not submitting for examination the pus from an abscess in this region, particularly in an individual not suspected of tuberculous infection. It has been my misfortune to find many such unsuspected cases were tubercular on later examination and I have been well pleased to have treated them with nitrate of silver as a routine protective agent. The silver salts undoubtedly tend to destroy the tubercle bacilli and do so without an extensive destruction of the underlying tissue, thus leaving the barrier Nature has previously thrown around the abscess and fistulous tract to protect the patient against further infection.
The wound should be thoroughly dilated with the finger prior to the treatment, in order to break down adhesion at the sides which leave areas higher up unhealed. In other words the granulating process must be permitted to advance only at the bottom of the wound so as to prevent the formation of a fistulous tract which might be covered by the healthier granulating surfaces near the skin.
Continue to:

My Books

