Abscesses. Part 2

Description
This section is from the book "Diseases Of The Rectum And Pelvic Colon", by Martin L. Bodkin. Also available from Amazon: Diseases of the rectum and pelvic colon.
Abscesses. Part 2
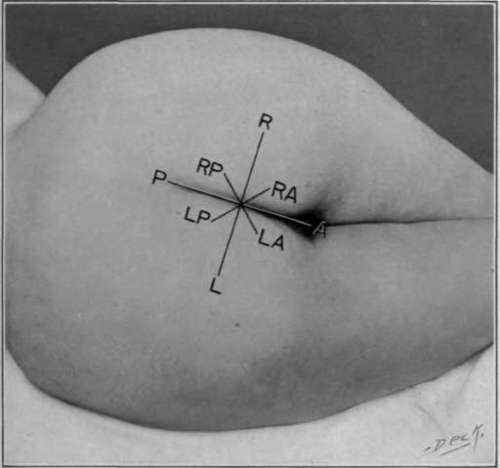
Fig. 50. Subdivision of perinea space (schematic).
"For convenience in describing the exact position of diseased conditions in relation to the anal margin and rectal wall, we have adopted the scheme of subdividing the perinea space into quadrants by two imaginary straight lines intersecting at right angles in the center of the anal aperture. The first line is drawn from the most prominent part of one tuber mischief to the other. This line we have termed the transverse anal line and by it the anal ring is divided into an anterior and a posterior half. When dealing with the various diseases met with in the rectum and anus, we shall endeavor to show that this line is of much clinical importance. The second line runs along the median rape from the tip of the coccyx to the symphonists pubis and intersects the transverse line at its center. We have designated the extremities of these lines by the letters, A, L, P, and R, representing respectively the anterior, left posterior and right points of the circumference of the anew-rectal region.
"Each of the quadrants is again bisected by two additional lines drawn at right angles to each other and intersecting the point of section of the lines AP and RL. The extremities of these lines are designated by the LA, LP, RP and R A. representing the left anterior, the left posterior, the right posterior and the right anterior quadrants.
"By adopting this scheme, the exact position of the disease can be definitely indicated. Thus an internal pile situated in the right anterior quadrant of the rectum can be briefly described, as the RA internal pile and similarly the external opening of a fistula situated posterior to the transverse line to the right side and distant from the anal margin say one inch may be readily described thus - external opening RP, one inch. This abbreviated and concise method of description is applicable to all other forms of disease met with in this region.
"Abscesses which start in the mischief-rectal Fosse, anterior to the transverse anal line, are more superficial in their course than those starting posterior to that line. In these, the pus reaches the subcutaneous tissue at the outer margin of the external sphincter muscle and then extends forward beneath the skin towards and along the Crusoe-scrotal or Crusoe-labial fold. At the same time burrowing takes place in an outward and backward direction, usually, superficial to the inferior hemorrhoid artery. The pus reaches the rectum between the internal and external sphincters at a point situated midway between the transverse anal line and the anterior margin of the anus, on the side on which the abscess exists. The internal opening may be situated at a point corresponding to the interval between the sphincters, but sometimes it may be quite an inch or even more above this point in consequence of the burrowing having extended upwards beneath the mucous membrane before bursting into the rectum. In such cases the burrowing may also extend even higher than this opening, a pocket being formed beyond it. Occasionally, the forward burrowing passes subcutaneously in front of the anus to the opposite side, thus forming a subcutaneous anterior horseshoe fistula."
Symptoms. The general symptoms are the sudden onset of the formation of pus, as occurs with ordinary abscesses. This may be marked by chills, rise in temperature, quickened pulse and pain, varying in degree according to the location and extent of tissue involved. The follicular abscess being so superficial, is marked by hardly more than itching, redness and discomfort in sitting. The mischief-rectal abscess is often attended with retention of urine and a feeling of weight in the rectum. When these abscesses burst into the rectum all the symptoms improve. Should the abscess cavity refill all the symptoms recur with the exception of the retention of urine. Often a history will be elicited which covers repeated refilling of such abscesses at periods for years.
Treatment. Many of these abscesses of subcutaneous variety yield readily to the application of carbolic acid, neutralized with alcohol. Should the abscess have burrowed, or originated in the subcutaneous tissue, it is much more satisfactorily incised under local anesthesia, in the form of ether spray, liquid air. ethyl chloride, cocaine, eucalypti or quinine and urea hydrochloride. The incision should be of the T-shape, with top of the T toward the anal opening to ensure free drainage and to permit granulation from the bottom of the wound.
Sub mucous Abscesses require, as a rule, dilatation of the sphincters and therefore necessitate the use of a general ansthetic Incision should be carefully made through the entire length of the abscess, parallel with the long axis of the rectum, in order to avoid the later accumulation of pus in a poorly drained pocket.

Fig. 51. Rectal abscesses. A, mischief-rectal abscess; B, sub mucous abscess.
A sub mucous abscess of the Y-shape, situated posterior and extending beyond a complete fistula, is of quite common occurrence and remaining undetected results in a failure to cure. When the burrowing has extended for a distance more than three inches up the rectum,care should be exercised to avoid penetrating the peritoneal cavity. Bleeding after primary incision of these abscesses is usually quite free and often requires firm packing.
Mischief-rectal Abscesses require free incision to drain the cavity, as well as to make a wide-open wound. The T-shaped incision is recommended for this purpose. The wound should be irrigated, curettage and entirely emptied of pus and necrotic tissue. The cavity should be cauterized with carbolic acid or tincture of iodine. Should carbolic acid be used, it is well to neutralize with alcohol, if the abscess cavity is very large, to avoid the poisonous effects of the acid; then pack the wound with gauze for two days. These sinuses are best treated without packing subsequently.
Continue to:

My Books

