Carcinoma. Part 11

Description
This section is from the book "Diseases Of The Rectum And Pelvic Colon", by Martin L. Bodkin. Also available from Amazon: Diseases of the rectum and pelvic colon.
Carcinoma. Part 11
Separation of rectum from vagina opening inducing the sphincters. The wall of the vagina is then dissected from its attachment to the rectum, exposing the rectum to full view and examination. The anterior wall of
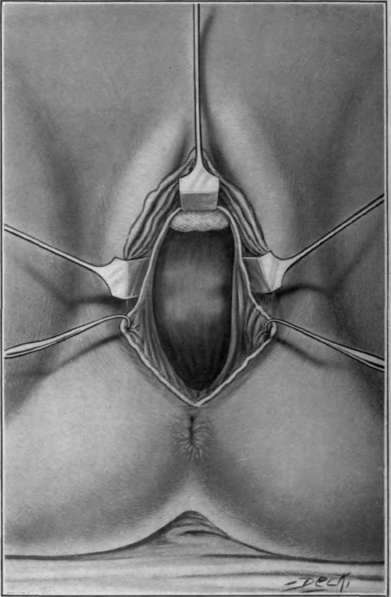
Fig. 85. Vaginal extirpation of rectum. Rectum cut open below neoplasm.
The growth is then amputated and the Upper and lower segment are united, end to end, by silk sutures, which should be passed from without inward,the knots tied upon the inside and the ligature left long enough to permit their easy removal. The anterior rectal incision should he closed in the same way, the sutures passed from without inward and the ligatures left long. The sphincters should be brought together by buried catgut sutures introduced in the same manner.

Fig. 86. Vaginal extirpation of rectum.
The peritoneal incision should be closed with continuous catgut sutures and the vaginal wound united with silk catgut sutures. A rubber drainage tube should be introduced through the rectum above the point of Anastasia and sutured into position. The external parts and the vaginal wound should be dressed with dry sterile gauze.
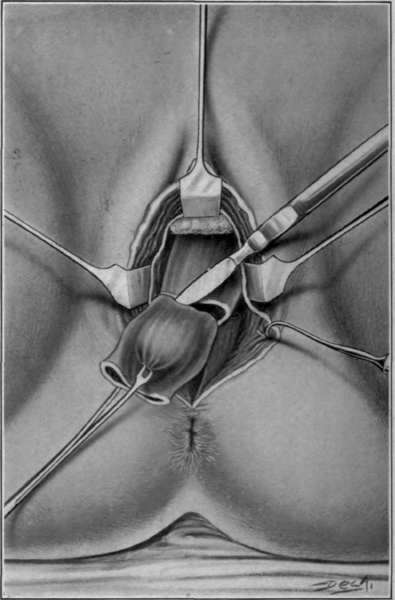
Fig. 87. Vaginal extirpation of rectum.
Excision of diseased area the rectum is then divided from the anal opening up to within one inch of the tumor. At this point a transverse incision is made through the entire gut, including the retro-rectal tissue. The upper segment of the gut is then closed with forceps and its posterior attachments are separated as far up as the promontory of the sacrum or so far as will permit the
Cuttle varies the technique of Murphy by commencing the operation with a muscular incision between the anus and coccyx, extending it into the retro-rectal space with the idea of permitting adequate drainage should infection occur at the point of Anastasia, or in the pouch of Douglas. After this incision has been made, the sacral cavity is packed with chloroform gauze to control oozing. The vaginal portion of the operation as conducted by Murphy is then completed excepting the gut is not cut across until it has been freed from all its attachments and the peritoneal cavity closed by sutures or firm packing.

Fig. 88. Vaginal extirpation of rectum.Suturing of rectum growth to be drawn down, to get sufficient healthy tissue for union with the lower segment.
Too much emphasis cannot he laid upon this suggestion for closing the peritoneal cavity at the earliest possible moment, as surgical work in this region is attended with danger of infection from the communist colt bacilli and other germs. It is probable that the mortality of the operation will always be high until our technique is so perfect as to offset infection of the peritoneum by introducing the finger into the peritoneal cavity at this point, or by the mere presence of the bacteria in the wound. The most careful and skillful operative technique during the other portion of the operation is lost and death may follow unless the strictest sepsis in manipulating the peritoneum at this point is observed.
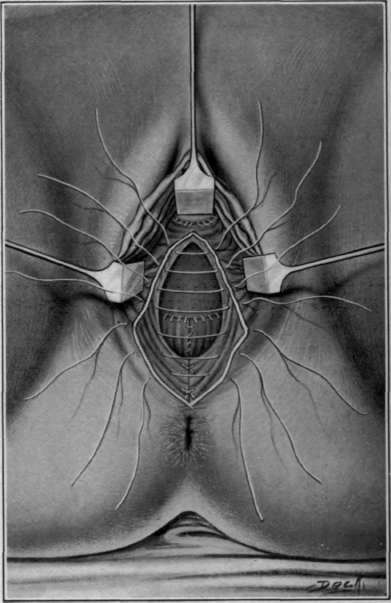
Fig. 89. Vaginal extirpation of rectum. Closure of vagina and peritoneal cavity.
Continue to:

My Books

