Carcinoma. Part 7

Description
This section is from the book "Diseases Of The Rectum And Pelvic Colon", by Martin L. Bodkin. Also available from Amazon: Diseases of the rectum and pelvic colon.
Carcinoma. Part 7
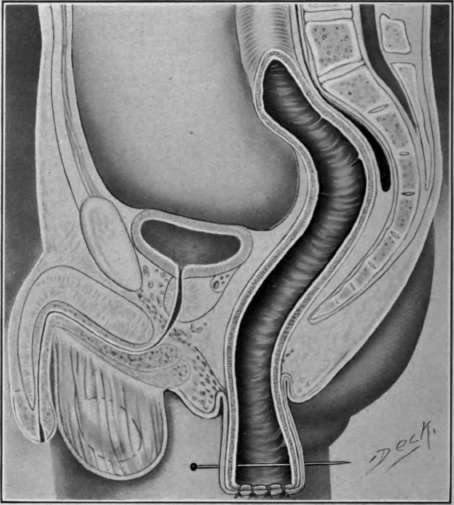
Fig. 75. Ab domino-anal extirpation.
Weir's method-sigmoid sutured to the peritoneal cavity is closed, and afterward the abdominal wound. He completes the operation by an incision posterior to the anus, extending into the pelvic space to the former position of the tumor, to allow drainage through a rubber tube. He also introduces a rectal tube wrapped with chloroform gauze to permit the escape of gas and prevent the bowel contents from coming in contact with the line of sutures.
Preparation of the patient for the combined abdominal perinea operation'. Patients often present the symptoms of toxemia, the result of prolonged partial intestinal obstruction associated with bacterial infection at the site of the malignant growth. The changes which take place in the blood and tissue from the toxemia produce in their turn, anemia, debility and loss of flesh. Thus some attempt should be made to relieve the over-burdened system by clearing the intestinal tract, and by forced feeding to improve the vital force necessary to withstand the operative shock. Ordinarily a week should be taken for accomplishing this task which should include the feeding of the patient at four-hour intervals. A mixed diet of meat, milk, broths, cereals and bread is superior to a milk diet on account of the constipating effect of the latter.
The mixed diet is more easily digested and permits forced feeding, thereby aiding in keeping the intestinal tract in proper condition. While the patient is undergoing forced feeding, a laxative should be given each day to produce two or three loose movements to offset intestinal auto-intoxication and relieve the system of its previous evil effects. Disinfection of the intestinal canal may be produced by the administration of either of the following well-known drugs: polycarbonate of zinc, two and a half grains; salon, ten grains; naphthalene, fifteen grains in capsules; or naphtha, ten grains. Either may be given three or four times a day.
During the four days previous to the operation the rectum should be washed out through a double current rectal irrigation three times a day with one of the following solutions: dichloride of mercury. 1-5000; permanganate of potash, 1-1500; or peroxide of hydrogen, three parts of sterile water to one part of peroxide of hydrogen.
The day previous to the operation and after the ordinary preparations have been made, the perineum and sacral region should be dressed with a soap poultice for two hours, then removed and the parts again washed, and finally a dichloride applied to be retained until the patient is anesthetized the following day. To further assist in an attempt to free the parts from bacterial life, the rectum should again be irrigated just before the operation, through a double current rectal irrigation, with a three per cent. solution of formalin, which should be wiped out. After this two or three ounces of pure peroxide of hydrogen should be injected into the rectum, above the tumor if possible. This procedure is intended to sterilize the parts should it be necessary to introduce the finger into the bowel, or it becomes necessary to perforate it in order to secure an imagination Every effort should be made to lessen the dangers of bacterial infection in this region, and it might be well to emphasize here, that such precautions should be rigorously instituted in all rectal operations which may inadvertently involve the peritoneal cavity.
The technique of the Tattle abdominal-perinea operation is as follows: The Brandenburg position is advised, to facilitate a clear view of the rectum and lower sigmoid in the abdominal cavity as well as to prevent the encroachment of other parts of the intestine into the field of operation. An incision is made on the outside of the left rectums muscle, beginning just below the umbilicus and extending within two inches of the symphonists pubes. This incision should avoid, if possible, the inferior gastric vessels and injury to the bladder. After the abdomen has been opened a sesrch may be made for metastatic involvement of the lymphatics and the location, extent, and the degree of involvement with the neighboring organs observed. Cuttle emphasizes that adhesion to other pelvic organs do not mean a malignant involvement of them and claims that some of his best results have been obtained in cases where the bladder and prostate have been attached to the growth, and further, that enlarged lymphatics do not always mean involvement in the pathological process. When adhesion plainly demonstrate the spread of the disease to the uterus and its appendages, these organs should be removed before operation upon the rectum, as it gives more room for that particular work, without adding too much to the entire operation.
Treatment of the sigmoid dysentery After determining the extent and involvement of the growth, a point is selected about two inches above the tumor, so as to allow that much extra tissue to make a new rectum after extirpation of the
The fat and glands should be removed from the blood vessels toward the gut until the lower sigmoid artery is discovered and traced to its origin in the superior hemorrhoid artery. Just above the lower sigmoid, the superior hemorrhoid artery should be tied with two ligatures and cut be twenty them. The lower sigmoid artery is usually found just below the promontory of the sacrum within the angle of the ilia vessels. This procedure provides for an Anastasia at whatever portion of the gut the amputation is made. The deep fascia behind the lower stump of the ligated vessel is split and the fat and glands at the side of the rectum down to the sacral cavity and to the tip of the coccyx posterior and the upper surface of the elevator an on both sides are cleared out. This cavity is then packed with moist hot pads to control oozing if present.
Continue to:

My Books

