Incomplete Prolapse

Description
This section is from the book "Diseases Of The Rectum And Pelvic Colon", by Martin L. Bodkin. Also available from Amazon: Diseases of the rectum and pelvic colon.
Incomplete Prolapse
Prolapses Mucosa Recto The connective tissues and sub mucous tissues of the rectal wall in health is held so loosely that a certain amount of sliding downward or an exaggerated version is easily permitted. In that way, a somewhat permanent laxity or elongation of the normal mucous membrane may take place, which in course of time or from the causes hereafter mentioned, produce an incomplete prolapse of the rectal mucous membrane. This form of prolapse is the most frequent, and occurs constantly as the result of any acute inflammatory process resulting in edema, hemorrhoids or acute proctorial
Causes of Incomplete Prolapse. Vesicular calculus, animosity,whooping cough, polyp, constipation, and undue straining are all responsible in some instances for the onset, or the continuance, of an incomplete prolapse of the rectum. Rectal prolapse is a positive index of a low vital condition, excepting when a definite history of a fall or other traumatize can be obtained, particularly in children.Sex Males seem to be more frequently afflicted with incomplete prolapse than females.
Age. Individuals of any age suffering from diarrhea, or who lack sphincter tone which permits a sagging of the mucous membrane are often afflicted for a long time after the subsidence of the exciting causes.
Occupation. The question of occupation as a cause of prolapse in children is generally eliminated, excepting in those permitting or required to carry burdens beyond their strength, which might easily be sufficient cause to originate or loosen the whole structure of the lower rectum.
Improper feeding during infancy is probably a more frequent factor in the cause of prolapse in either the adult, or child than is credited. A direct line of questioning the adult will often elucidate the vague or meager history of attacks of incomplete prolapse during childhood.
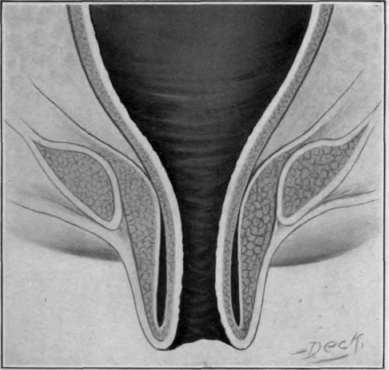
Fig. 28. Complete rectal prolapse, first degree.
Symptoms. There is a protrusion, which is either lateral
As a rule these cases do not protrude more than two and one-half inches; there may be little pain and the condition appear to be nothing more than an exaggeration of the normal version of the rectal mucous membrane which occurs at every stool. At first the prolapse is easily reduced, or it may recede without pressure but as the mucous membrane grows thicker from the inflammatory process, sphincter contraction prevents its recession.
My opinion is that children seldom suffer from any form of hemorrhoids excepting the thrombotic and nae void and that supposed hemorrhoids are a part or wholly a prolapse of the mucous membrane.
Diagnosis. The diagnosis between complete and incomplete prolapse is a matter of importance in children only. An incomplete prolapse in the adult is insignificant as to danger. The diagnosis of the complete variety is easily made in adults because the muscles and tissues are so developed that the circular fibers of the rectal wall are recognized by their crescent folds. The incomplete variety seldom exceeds two inches, and one side is generally longer than the other. In the complete variety, the protrusion is generally equal on all sides of the circumference, measuring from two to four or five inches in length in adults, as a rule.
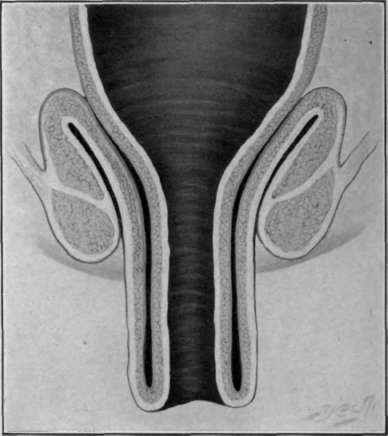
Fig. 29. Complete rectal prolapse, second degree or bilateral, a discharge of mucus, often loss of control of the sphincters, increased frequency of parturition and bowel movements, and there may be hemorrhage, and a dragging sensation.
In incomplete prolapse, the aperture is generally oval or circular and in the middle of the protrusion. In the complete variety, the aperture is oval or crescent and pushed backward, because the mes-rectum holds the rectal wall posterior In the incomplete variety there are almost invariably well-marked sulfide, anterior and posterior; and in this variety there are only two layers of the mucous membrane and the sub mucous tissue contained in the protruding mass. In the complete, the mass contains two layers of mucous membrane, two layers of sub mucous tissue, and four muscular coats which form a solid mass by comparison to the incomplete.
Palliative Treatment. In the treatment of incomplete prolapse one should hold in mind that it is simply a sliding down of the mucous membrane, and that in children the constitutional condition is probably the underlying cause, no matter what may have been the exciting cause. A chronic diarrhea, or any one of the enumerated causes, may have been the original trouble, leaving a loss of tone or an atrophy of the muscle, permitting sliding down or relaxation of the mucous membrane.Palliative treatment may be tried when the prolapse is of short duration and slight in degree, but otherwise surgical treatment should he instituted to obviate the danger of strangulation.
Reduction after each movement of the bowel is important, and should be done as soon as possible after the protrusion has occurred. For this purpose the thumb or small finger should be bound around with absorbent cotton slightly oiled, and pressure made steadily and gently into the lumen of the gut. The patient should be placed upon the side, or in the knee-chest position, and the mass pushed beyond the upper border of the internal sphincter. After reduction the patient should remain in the prone position for at least a few hours. The application of the method suggested by Powell of strapping the buttocks after reduction is oftentimes successful. The strapping should be done with the child lying on its side, and with three-inch adhesive straps, passing from one trochaic to the other, drawing the buttocks close together and folding them in. The posterior edge of the adhesive strap should only reach as far front as the anterior edge of the anus. The straps applied in this manner will allow defecation and necessitate removal only once a week. Defecation should be permitted only while the child is on its side or in the recumbent position. Children under three years of age should be held in the vertical position while defecating, to avoid straining. It is very important that the food should be made as near perfect as possible, and the child kept out of doors for the benefit of fresh air and exercise. Should constipation exist, it is best treated with cascara, cod liver oil, or with olive oil. As a general tonic and laxative the following will prove of value.
Continue to:

My Books

