Malformations. Part 3

Description
This section is from the book "Diseases Of The Rectum And Pelvic Colon", by Martin L. Bodkin. Also available from Amazon: Diseases of the rectum and pelvic colon.
Malformations. Part 3
The operation of Grizzlies recognizes the sphincter action at the vaginal anus and takes the tissue as a whole and aims to preserve it after removal to the normal anal site. His operation is as follows: An incision is made from the posterior margin of the vagina to the site at which the normal anus should have been. A careful diagnosis is then made to reach the rectal pouch which is loosened from its attachments, the vagina] anus is then dissected out and dragged down to the normal position of the anus.
The vagina and perineum previously cut through are then sutured together with either catgut sutures or deep silver sutures and the mucous membrane is restored, which then completes the recto-vaginal septum. In cases where there have been two openings into the vagina, a plastic operation is necessary which will require great ingenuity in order to accomplish good results. When two openings exist, single incisions which convert the two into one opening, the margin surrounded by a purse string suture, and sewed into the normal side of the anus, will often prove successful. When the openings are widely separated it is a better plan to use the lower opening for the new anal canal and close the upper opening by inversion with Lambert sutures.
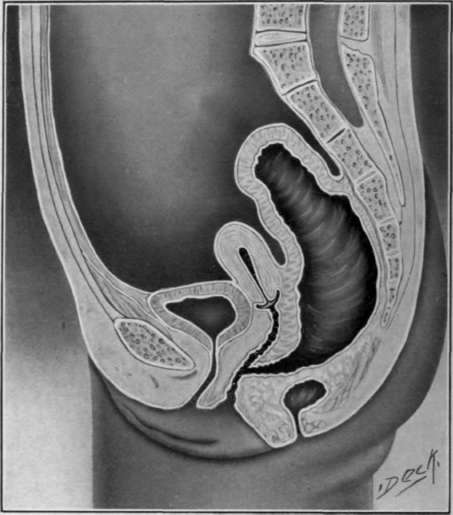
Fig. 11. Atreus an vaginal is.
Atreus Agni Uterine. This communication is probably of the rarest variety. The malformation is so infrequent that little is known of it and no definite plan of treatment has been laid out. The life of the child should be the first consideration, which would dictate either a colostomy, or, if possible. the establishment of the anus at the normal site.
Normal Anus with Some Other Viscus Opening into the Rectum. When the uterus or vagina opens into the rectum the course of treatment described for Atreus Agni Vaginal is would apply. When the ureters empty into the rectum, the bladder is absent and are beyond surgical aid, eventually leading to infection and death from kidney abscess.
Complete intestinal obstruction
These malformations are of four different types:
1. Complete occlusion of the anus.
2. Entire absence of the anus.
3. Rectum arrested in its descent.
4. The entire absence of the rectum.
Complete Occlusion of the Anus. The difference between the complete occlusion and the partial occlusion of the anus by a membrane or diaphragm is one of degree only. The partial occlusion may not be in any way dangerous to life, but when this band is composed of fibrous or much-cutaneous tissues thick enough to cause total occlusion, the child's life must be saved by the immediate relief from the obstruction. Partial occlusion occurs more often than statistics show, as the physician in attendance usually provides a free exit for the zirconium as soon as the malformation is observed.
When the rectum has properly developed, the zirconium can be easily seen pressing against the thin and transparent membrane. The question as to whether this malformation results from an arrest in the absorption of the membrane dividing the rectum and anus during its embryo logic formation, or during the development of the rectum from the hypo blast and fibroblast, is still one of doubt. In some cases the membrane bridges over the skin, and in others is located high up in the anal canal, at or at about the pectin, which would suggest that it is due to an arrest in absorption, but does not explain why it occurs in the lower position. Therefore, we have either a malformation, or unabsorbed tissue resulting in a deformity.
Simultaneous with the development of the rectum, there is an imagination or turning in of the echinoderm, fibroblast or serous layer which persists until absorbed. The proctorial of the fibroblast and the hypo blast (echinoderm or mucous layer) approach each other forming a double septum between the rectum and anus. The absorption of this membrane completes the anal and alimentary canal.
The absence of the natural discharge of zirconium will be the first symptom observed, the bulging, discoloration of the membrane, and the inability to introduce the finger into the rectum will corroborate the diagnosis.
A complete occlusion by a membranous band is best treated by a crucial incision and subsequent dilatation with the finger as suggested for the abnormal narrowing. Care should be exercised that the cicatrix resulting from cutting the membranous band does not contract.
Entire Absence of the Anus. This malformation is comparatively rare, per SE. As a rule it presents only a slight DE precision in the skin, where the normal anus should be; or there may be a slight elevation of skin or a protrusion at this part. The most pronounced observation in some cases will be that the rape in the perineum may extend all the way from the scrotum to the coccyx. In some cases there may be a slight discoloration over a partly formed anal ring.
These cases may present almost the same symptoms as the condescended rectum, when the rectum reaches close to the skin. There may be an condescended rectum, a malformation of hypothetical origin, or an absence of the anus of neoplastic origin. In those cases in which there is simply an absence of the anus, we would expect to find the rectum normal in its descent to the pectin, and surgical procedure would not be so dangerous: whereas the other condition - the condescended rectum-would necessitate one of the severest surgical priced-ures in this region.
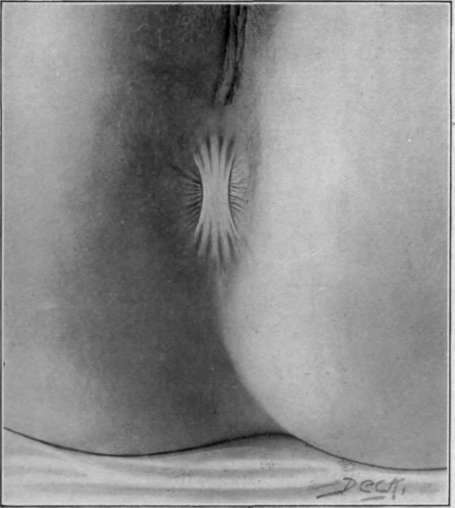
Fig. 12. Membranous occlusion of the anus.
Rectum Arrested in its Descent. In this form of malformation the rectum is either arrested in its development and fails to reach the anal opening, or it may descend in the wrong direction and fail to reach the anal canal. The rectum may he arrested at a variable distance from the anus, sometimes only within so short a distance as to suggest the complate occlusion by a membranous band, while in others several inches may intervene. There may be obstructions at several points due to adhesion above the condescended rectum.
Continue to:

My Books

