Structure Of The Rectum. Part 4

Description
This section is from the book "Diseases Of The Rectum And Pelvic Colon", by Martin L. Bodkin. Also available from Amazon: Diseases of the rectum and pelvic colon.
Structure Of The Rectum. Part 4
The after-treatment of posterior proctorial should consist of a daily flushing out of the rectum and every precaution to keep the wound healthy. Tincture of iodine, balsam of Peru, nitrate of silver and naphthalene solutions will be found of great service. During the treatment a large sized bogie should be passed occasionally to prevent the recurrence of the stricture.
Total excision was presented as a most enticing operation for the relief of stricture some years ago, but has proven to be unreliable and subject to sepsis, abscess, fistula and death. The sutures used to unite the bowels are subject to infection and are likely to separate, causing another stricture. The perinea and sacral methods are advocated in performing this operation. The technique is the same as for malignant growths, which may be modified for the special indications.
Bacon's operation for performing a lateral enter-anas-tomosis has proved a most ingenuous method for the relief of the structure of the rectum situated above the elevator an muscles. The operation, as the name indicates, consists in making a lateral opening between the rectum and a duplication of the sigmoid flexible below the stricture.
The technique is as follows:The patient is placed in the Brandenburg position and an incision made from the umbilious to the pubis, and after entering the abdominal cavity the sigmoid is folded downward until it reaches below the stricture. This measures the point at which the lateral Anastasia is to be made. This portion of the sigmoid is then brought Up and out of the abdomen and. with Morphyâs clamps above and below the point, a longitudinal incision is made through the gut between the clamps and the male half of a Moor phys button secured in this incision. The peritoneal surfaces of the sigmoid and rectum which are intended to be put into apposition later are scarified and the female portion of the button introduced into the wall of the rectum with the short trochaic made for that purpose. This should be accomplished by passing the trochaic in the instrument through the hole in the button, then it is pushed up into the rectum by an assistant to the point below the stricture. The operator at the same time presses down upon the trochaic from the peritoneal side and forces it to penetrate the wall, carrying the neck of the button with it. The ends of the button are then approximated by the operator and the lateral Anastasia is made complete. A few sutures should be placed in the peritoneal gut of the folded sigmoid to prevent any small loop of the intestine from coming down between the sigmoid and rectum, and also to strengthen the Anastasia If the operation has been done without any leakage from the rectum or the sigmoid into the abdominal cavity, the abdomen may be closed and primary union looked for. The Murphy button will be expelled in five to eight days. After expulsion of the button, a rectal enema should be given and the colon emptied. Within a few days or as soon as the comfort of the patient will permit a long clamp should be inserted through the rectum and one blade introduced through the buttonhole into the sigmoid, while the other extends up the rectum so as to include the stricture. The septum is then completely severed by closing the handles a little tighter each day.
By this procedure the caliber of the gut will be increased to that of the sigmoid flexible colostomy. When stricture of the rectum or lower sigmoid is inoperable by either excision, proctorial or dilatation a colostomy is resorted to. The establishment of an artificial anus is also resorted to when either of these operations have been done and the stricture recurs, or when symptoms of auto intoxication or infection are so pronounced as to threaten life and it becomes imperative to give free vent to the intestinal contents.Colostomy allows an opportunity of treating the structured through nonautomotive opening and stricture to widen it by pressure necrosis portion of the gut from both sides; allows complete drainage of the intestinal tract; relieves distention, irritation and obstruction to the fecal current; so that the establishment of an artificial anus has many good points when circumstances render the operation necessary. While the operation is condemned by many surgeons, misery and death can often be avoided for a long period by this procedure. The technique of the operation will be found under Chapter IX (Colostomy).
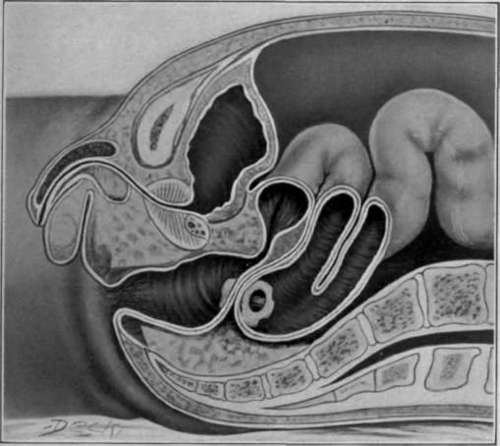
Fig. 55. Stricture of rectum. Bacon's lateral Anastasia

Fig. 56. Trochaic for insertion of female segment of Morphyâs button in Bacon's operation for stricture of the rectum.
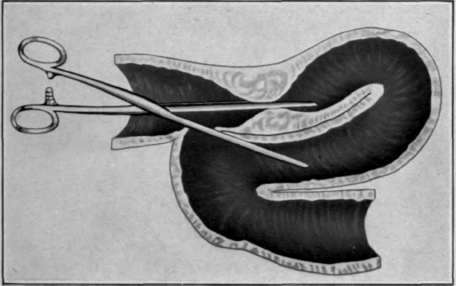
Fig 57. Bacon's operation-Clamp
Continue to:

My Books

