Carcinoma In Situ
Description
This section is from the book "Early Detection And Diagnosis Of Cancer", by Walter E. O'Donnell. Also available from Amazon: Early Detection And Diagnosis Of Cancer.
Carcinoma In Situ
Before proceeding to a discussion of the pathology of invasive cervical cancer, it is essential to deal with the concept of carcinoma in situ. This is also called intraepithelial, and sometimes preinvasive, cancer.
There are many definitions of the term carcinoma in situ, none of which has gained universal acceptance. In general, it is a microscopic diagnosis that is applied to certain histologic changes of cancer occurring in the epithelial cells of the cervix without any demonstrable evidence of invasion of adjacent tissue. The precise criteria by which one makes this diagnosis and particularly the distinction between some of the major cytologic atypias and actual carcinoma in situ, as well as the dividing line between frank carcinoma in situ and the earliest stage of invasive cancer, are the subject of continuing debate. In this setting, the clinician's major responsibility is to submit the cytologic and pathologic material to a competent cytopathologist and be guided by his findings.
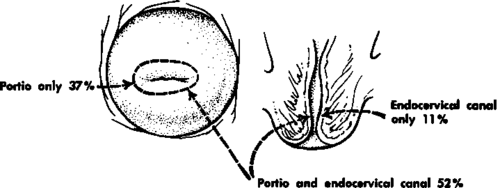
Fig. 51. Distribution of in situ carcinoma of the cervix. (From Foote, F. W., and Stewart, F. S.: The Anatomical Distribution of Intraepithelial Epidermoid Carcinomas of the Cervix, Cancer 1:431-440, 1948.).
Carcinoma in situ of the cervix was first described almost fifty years ago, but for years it remained more of a pathologic curiosity than a clinical problem. In the past fifteen years or so, however, the advent of widespread application of the study of the exfoliative cytology of vaginal and cervical smears by Papanicolaou and related techniques has completely changed things. Cytologists, pathologists, and clinicians are making the diagnosis of carcinoma in situ of the cervix with increasing frequency. There has been much debate about the nature and management of carcinoma in situ as well as about the very important question of its relationship to invasive cancer.
The consensus with regard to the nature of in situ cancer might be summed up rather arbitrarily as follows:
1. It is actually cancer, even though it may lack one of the conventional hallmarks of the disease (i.e., invasiveness). It should not be regarded merely as a premalignant lesion.
2. Some-but by no means all-carcinoma in situ lesions may progress to become invasive cancer. Estimates vary widely. Some believe that most such lesions will do so if untreated; others believe that very few will. At present it is probably wise to regard this as an unanswered question. Some tentative conclusions may be possible in the next few years as the results of long-term follow-up studies become available.
3. Most, if not all, invasive cervical cancers go through an early phase of carcinoma in situ. It is possible to detect them at this stage by cytologic techniques. Furthermore, it appears that there may prove to be different grades of carcinoma in situ.
4. Contrary to expectations, the lime that it takes for the average lesion to progress from carcinoma in situ to invasive cancer is quite long. The difference in the average age of patients at the time of diagnosis of the in situ and invasive lesions (less than 40 years vs. 46 years), as well as those cases in which the transition has occurred while the patient was under continuing observation, suggests that it may be well over six years. During all this time it is a readily detectable, curable lesion.
5. Although the in situ lesion may progress to invasion, it also may remain stationary, regress, or disappear spontaneously. Also, the so-called major atypias have been observed to progress to carcinoma in situ.
6. There is no precise way of separating the indolent from the potentially aggressive lesion.
7. Some of the cytologic atypias discovered on vaginal or cervical smear may be the precursor of carcinoma in situ, although more precise definition is needed on this point.
If one accepts the concept of cervical cancer just outlined, it is apparent that some basic reorientation of thinking regarding the detection, diagnosis, and management of the lesion may be required.
In the first few years following its introduction, some disrepute was cast on the concept of the in situ lesion and the value of cytology by some physicians because of an occasional distressing experience.
For example, a diagnosis of cervical cancer might have been made or suggested in the cytologic report. Attempts to confirm this change by biopsy then might have failed in a certain number of cases. Or, occasionally and regrettably, the finding of a positive or suspicious smear was used as the sole justification for hysterectomy-only to find no cancer in the surgical specimen. Experiences such as these suggested to some that cytology was an inaccurate technique, unsuitable for routine use.
In our opinion, such a conclusion is not warranted. We believe that a more critical and enlightened use of vaginal and cervical smears will obviate most of these difficulties and allow full use of this important screening technique.
Mistakes have usually been made in one of the following directions:
1. Overdiagnosis of carcinoma in situ. An earlier tendency to over-read the slides is being replaced by insistence on stricter criteria for the cytologic diagnosis.
2. Over-reliance on cytology. It has been found that misdiagnosis, especially false positives, can be kept to a minimum by requiring biopsy proof of all lesions.
3. Overtreatment. Relatively radical surgical or radiotherapeutic procedures have been justified by some on the grounds that the presence of cancer demands an all-out onslaught. Newer knowledge and more rational consideration of the matter have made it apparent that each case must be individualized and that considerable conservatism may be not only possible but also proper.
Continue to:
My Books

